Algoritm for Ankle Fractures 2.0
Frank Smithuis andRobin Smithuis
Radiology department of the Amsterdam University Medical Centre in Amsterdam and Alrijne hospital in Leiderdorp in the Netherlands
Publicationdate
In this lecture we present a simple algoritm that helps you to find:
- All ankle fractures, even the ones that are not visible on the X-rays
- Predict rupture of ligaments even if you can’t see them on the images
- Determine whether the ankle is stable or unstable, just by looking at the radiographs
The algoritm is based on the Weber-classification, because it is simple and everybody knows it. Since the Weber-classification is a simplification of the Lauge-Hansen classification, it will help you to understand the different stages of Lauge-Hansen.
Introduction
Algoritm for ankle fractures
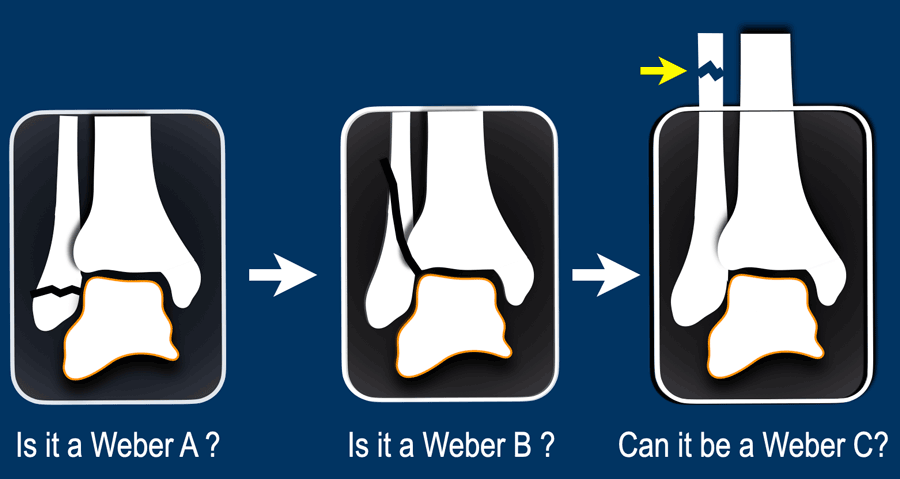
Step 1
The first question you should ask yourself is:
Is it a Weber type A fracture?
Is there an avulsion of the lateral malleolus. That’s easy.
Step 2
If it is not a type A. Then the next question is:
Is it a Weber type B fracture?
This oblique fracture at the level of the syndesmosis is always easy to find on the x-rays.
Step 3
If it is not type A or type B, then the last question is:
Can this be a Weber type C fracture?
These fractures are usually not visible on x-rays of the ankle, because the fibula fracture is too high, but the algoritm provides clues for the detection of these fractures.

When we've answered the above questions, then we end up in one of these three categories.
In each of these categories we need to determine the stage of the fracture, which tells us if the ankle is stable or unstable.
In Weber A stage 1 is stable.
However when there is also a vertical or push-off fracture of the medial malleolus, then it is stage 2 and the ankle is unstable, as the ring of stability is broken in two places.
In Weber B stage 2 is stable, but stage 3 and 4 are unstable.
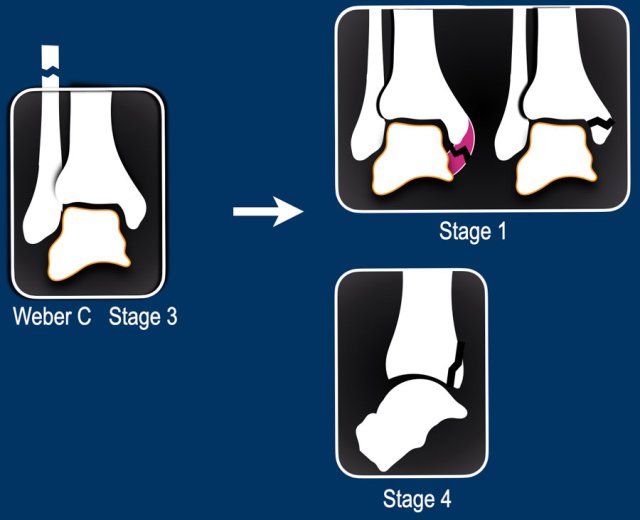
In Weber C finding a high fibula fracture means unstable stage 3. Since this fracture is usually not visible on x-rays of the ankle, you wanna study the ankle x-rays to look for stage 1 and 4, which can be a clue to image the whole lower leg to look for a high fibula fracture.
These stages in Weber B and C always follow a strict order.
This means that when you find a stage 3 fracture, there already must be a stage 1 and 2 even if you can't see them.
We will discuss these stages in the next chapter.
Fracture stages
This is an overview of the stages of ankle fractures. It was originally described by Christian Lauge-Hansen, a Danish pathologist in 1950 and later copied by Bernhard Georg Weber in 1972, a member of the AO-group.
Stages of Weber A
- Lateral avulsion
- Medial vertical push-off fracture
Stages of Weber B
- Rupture of anterior syndesmosis or less common Tillaux fracture (avulsion of tibial attachment).
- Oblique fibula fracture at level of syndesmosis.
- Tertius avulsion fracture or rupture of posterior syndesmosis
- Avulsion fracture of medial malleolus or rupture of medial collateral bands
Stages of Weber C
- Avulsion fracture of medial malleolus or rupture of medial collateral bands
- Rupture of anterior syndesmosis or less common Tillaux fracture (avulsion of tibial attachment).
- High twist-like fibula fracture above the level of the syndesmosis.
- Tertius avulsion fracture or rupture of posterior syndesmosis
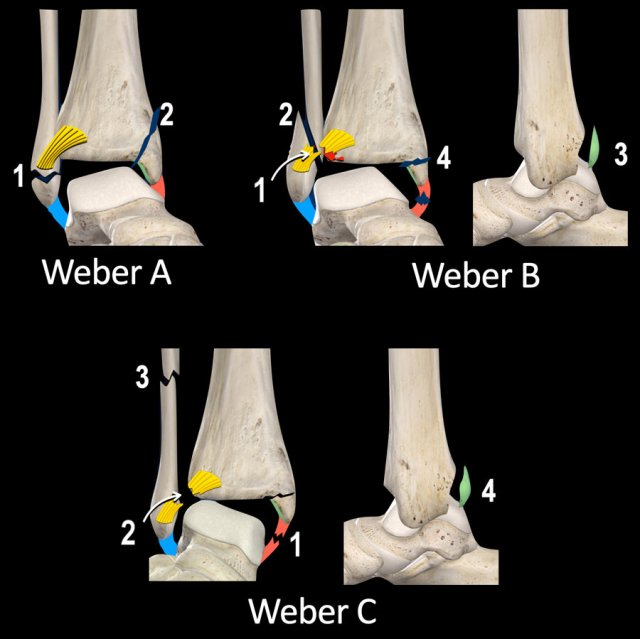
Weber B and Weber C fractures are very different in the type of fibula fracture.
In Weber B there is a oblique oriented push-off fracture at the level of the syndesmosis, while in Weber C there is a twist-like fracture above the level of the syndesmosis.
Notice however, that there are many similarities between Weber B and C with only differences in the order of events. For instance a tertius fracture is either stage 3 in a Weber B or a stage 4 in Weber C fracture.
Another important thing to realize is that traction on a ligament results in either a rupture of that ligament or an avulsion fracture at the insertion of that ligament.
Step 1 - is it a Weber A / SA
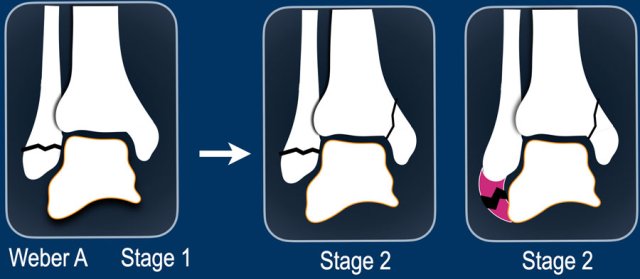
Weber A is the result of a pull-off or avulsion on the lateral side due to extreme supination of the foot with adduction. This is stage 1 and is stable.
Lauge-Hansen calls this supination-adduction (SA).
Although not that common, the injury may proceed and cause a push off fracture on the medial side resulting in a vertical fracture of the medial malleolus . This is always stage 2 and is unstable, whether you see a fracture of the lateral malleolus or not. In rare case you may find a vertical fracture of the medial malleolus in combination with a collateral band rupture on the lateral side.
 Stage 1: stable ankle fracture
Stage 1: stable ankle fracture
Stage 1
Here a typical avulsion or pull-off fracture of the lateral malleolus.
The avulsion fragment is quite large. More commonly there is a small avulsion fragment.
This is a stage 1 stable Weber A fracture.
Stage 2
This case is more challenging.
This fibula fracture is at the level of the syndesmosis and maybe some people would call this a Weber B fracture, but it doesn't look like a Weber B. A weber B fracture is oblique and more vertical because it is a push-off fracture, which we will discuss later.
Just by looking at the images, you can understand the trauma mechanism (scroll).
This is a stage 2 - unstable bimalleolar Weber A fracture.
The left image is another example of an unstable bimalleolar fracture stage 2 Weber A.
The right image shows a vertical fracture of the medial malleolus (arrow). This is always stage 2 and unstable. It means that there already is stage 1, because the trauma mechanism always follows this strict order, first stage 1 and then stage 2.
The ring of stability is broken in two places (scroll).
Step 2 - is it a Weber B / SER

If it is not a Weber A fracture, then the next question is: is it a Weber B?
When you see a Weber B fracture, which is always good visible on either the AP- or the lateral view, the only thing you need to check is whether there is an unstable stage 3 with posterior injury or even stage 4 with medial injury.
Weber B is the most common ankle fracture accounting for 60-70% of all ankle fractures.
Just like a Weber C fracture it is the result of an exorotation force applied by the foot.
The only difference is that in Weber B the foot is in supination and the injury starts on the lateral side where the tension is, while in Weber C the injury starts on the medial side due to the position of the foot in pronation.
Lauge-Hansen called this fracture mechanism supination exorotation or SER.
The fracture mechanism that leads to a Weber C fracture is called pronation exorotation or PER and we will discuss it in the next section.
Scroll through the images to see how the injury follows a clockwise fixed order.
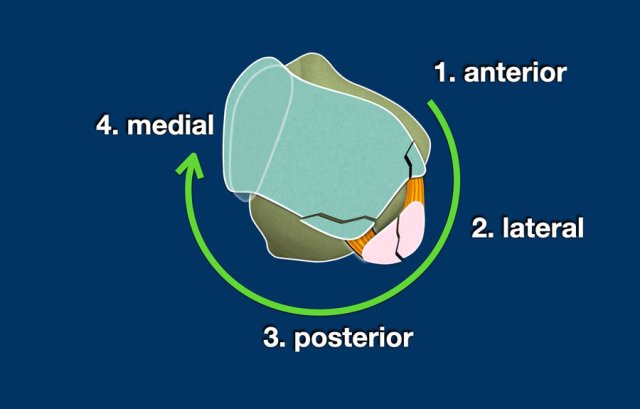
Things become very easy once you remember the fixed order of the injuries:
- Anterior
Tension in anterior syndesmosis results in rupture of the syndesmosis or avulsion of the tibial attachment - Tillaux fracture. - Lateral
Exorotational force on the fibula results in an oblique - push off fracture. - Posterior
As the talus pushes the fibula fragment in a posterior direction, the tension in the posterior syndesmosis will result in band rupture or avulsion of the malleolus tertius. - Medial
As the talus moves further away in a posterolateral direction, this will create enormous tension in the medial collateral band resulting in a band rupture or avulsion of the medial malleolus.

Tillaux fracture
The injury mechanism that causes a Weber B fracture can stop at any stage. Most commonly we see stage 2 which is the oblique fibula fracture, but sometimes the injury stops at stage 1.
Usually this is a rupture of the anterior syndesmosis and we don't see anything on the x-rays, but the patient will have a lot of pain on this specific anterolateral spot. The tension in the anterior syndesmosis can sometimes lead to an avulsion of the tibial attachment of the anterior syndesmosis, which is called a Tillaux fracture. An avulsion of the fibular attachment is even more rare.
Images
On the AP-view and the coronal CT-reconstruction we see a Tillaux fracture as stage 1. No other fracture was seen.

Study these images. You may have to click on them to get a larger view.
First Question: Is it a Weber A, B or could it be a Weber C? Then try to figure out the stage and determine whether the ankle is stable or unstable.
You can look at the next images for a discussion of the images.
Scroll through the images.
It is a stage 4 Weber B fracture, which is unstable.
Step 3 - Could it be a Weber C / PER
When the x-rays of the ankle show no obvious fracture like a Weber A or B, then the question is: could this be a Weber C fracture?
Since the fibula fracture in a Weber C is most commonly not visible on the x-rays of the ankle, this can be a tough question to answer.
We will have to look for additional findings that lead us to the right answer and that will help us to make the decision to do additional images
Since the fibula fracture is already stage 3, we wanna look for:
- stage 1 which is the medial injury, where it all starts. Any pain or soft tissue swelling on the medial side can be a first indication that we are dealing with a Weber C fracture.
- stage 2 is injury to the anterior syndesmosis, which is usually not visible, unless there is a Tillaux fracture.
- stage 4 is injury to the posterior syndesmosis, which sometimes can not be seen, but will be suspected if there is a widening of the ankle fork or when there is an avulsion of the malleolus tertius like we see in the illustration.
Mechanism of Weber C
The mechanism of a Weber C is a result of a position of the foot in pronation with an exorotation force applied by the foot and that is why Lauge-Hansen calls it pronation exorotation (PER).
The stages are:
- Due to the pronation there is enormous stress on the medial collateral bands and that’s where the injury will start with either a band rupture or an avulsion of the medial malleolus (stage 1).
- As the exorotation force continues the anterior syndesmosis will rupture (stage 2).
- As a result of the pronation of the foot, the bands on the lateral side are all without any tension. As the exorotation of the foot continues the distal fibula follows this exorotation movement, while the proximal fibula is held in position at the proximal tibiofibular joint and you get a twist-like fracture somewhere above the level of the syndesmosis (stage 3).
- And finally in stage 4 there will be a rupture of the posterior syndesmosis or tertius avulsion (stage 4).
In the axial plane you can see that the injury starts on the medial side due to the pronation of the foot and follows a clockwise rotation through anterior and lateral to posterior.
And just like in a Weber B, you can get injury to the anterior syndesmosis, fibula and finally the posterior syndesmosis.
The two differences between Weber B and C are:
- Weber B starts anterolateral due to the supination of the foot, while Weber C starts on the medial side due to the pronation of the foot.
- Exorotation of the foot in Weber B results in a oblique push-off fracture because the fibula is held against the talus due to the supination, while in Weber C the fibula is quite loose resulting in a twist-like high fibula fracture.

Sometimes we are lucky, because the fibula fracture is visible on the x-rays of the ankle.
Then we know we are looking at an unstable stage 3 weber C fracture.
In this case there is widening of the medial clear space between the medial malleolus and the talus indicating a rupture of the medial collateral bands (stage 1).
We have to assume that there also is a rupture of the anterior syndesmosis (stage 2).
There also could be a stage 4 injury to the posterior syndesmosis.
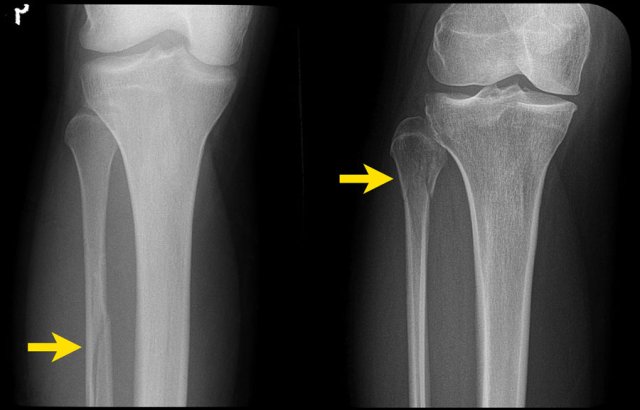
In many cases however, the fibula fracture is higher up and we need additional x-rays to find the fracture.
It is our job as radiologists to find clues on the x-rays of the ankle that will lead us to these high fibula fractures and the algoritm will help us.
 Click on the images to enlarge
Click on the images to enlarge
Study the images.
Use the algoritm and ask yourself if it is a Weber A or B or that it could be a Weber C.
Then determine the stage.
Then continue for a discussion of this case.
- At first sight it just looks like only a tertius fracture.
- When we look at the algoritm, you can see, that a tertius can be found in a Weber B fracture in stage 3 and in a Weber C fracture in stage 4.
Since this patient doesn't have a Weber B, it must be a Weber C fracture. An isolated tertius fracture is very uncommon and probably does not exist. - Now we recognize the soft tissue swelling on the medial side, which is stage 1.
- On the enlarge view we also recognize a small avulsion fracture.
Having detected stage 1 and 4 of a Weber C type of trauma mechanism, we now are sure that there must also be a stage 3, which is a high fibula fracture.

Charity
All the profits of the Radiology Assistant go to Medical Action Myanmar which is run by Dr. Nini Tun and Dr. Frank Smithuis sr, who is a professor at Oxford university and happens to be the brother of Robin Smithuis.
Click here to watch the video of Medical Action Myanmar and if you like the Radiology Assistant, please support Medical Action Myanmar with a small gift.