MRI examination of the Elbow
by Mark Anderson
University of Virginia Health Sciences Center
Publicationdate
This review is dased on a presentation given by Mark Anderson and adapted for the Radiology Assistant by Robin Smithuis.
We will discuss:
- Basic MR techniques and MR arthrography.
- Appearance of normal anatomic structures.
- Common types of pathology.
MRI technique

Scan planes
Just like in the shoulder you need to be sure to get the imaging planes correctly in a standardized way.
Use the axis of the epicondyles on a axial localizer to plan the coronal scan.
The sagittal images are scaned perpendicular to the coronal scan.
In this way you get very persistent images and you will get used to the normal anatomy.
Imaging sequences
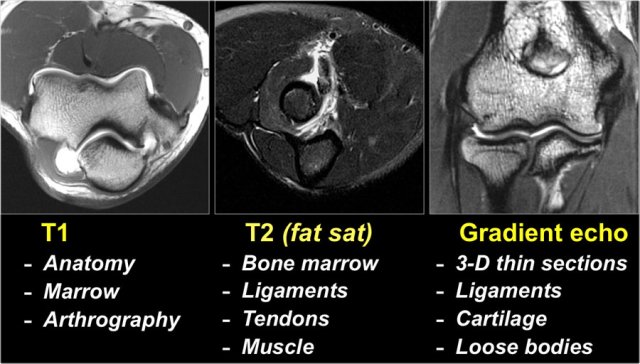
T1
In every joint that is studied you should have at least one T1-sequence not only to look at the anatomy, but also as a back up for looking at the marrow.
Ofcourse the T2-fatsat images will show marrow abnormalities, but T1 can be helpful in telling us what is really going on.
T1 is certainly used in MR-arthrography.
T2-fatsat
T2 will show us most of the pathology, whether it is in the bone marrow, ligaments or muscle because of the high water content. It can also be used to image cartilage.
Gradient echo
With gradient echo we can use 3-D thin sections to image the cartilage and the ligaments.

In the MR-protocol we do T1 and T2-fatsat in all three imaging planes.
Sometimes STIR is used.
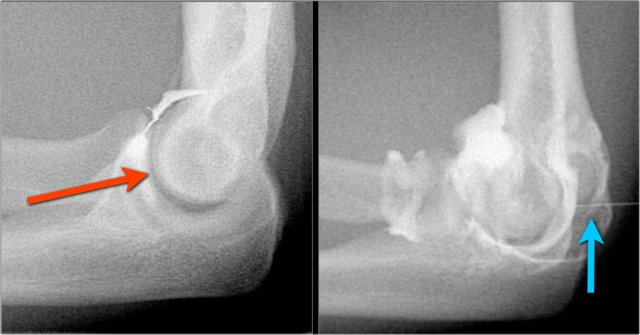
MR-arthrography
Typically the radiocapitellar joint is punctured from lateral with the patient prone and the arm flexed 90 degrees overhead (red arrow).
This however can sometimes cause problems if you are interested in the lateral ligaments and you inject lidocaine or contrast into these ligaments.
So more recently we started to use the posterior approach into the olecranon fossa (blue arrow).
Diluted gadolinium is injected, i.e. 0,05cc + 10cc saline (an "off-label" use in the US).
Indications for MR-arthrography are:
- UCL pathology in throwers.
- Osteochondral lesions and repair
- Loose bodies
Anatomy and Pitfalls
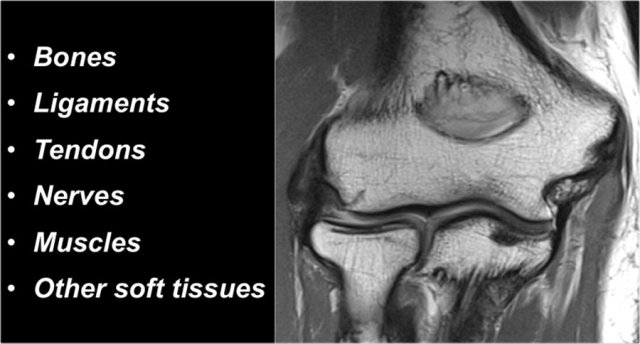
When you study the anatomy of the elbow, it is good to use the inside-out approach.
First study the bones and then continue with the ligaments and the tendons and then the surrounding structures.
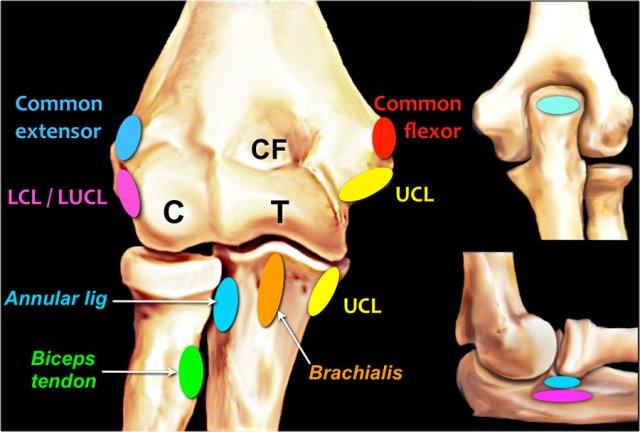
Tendon attachments
Common flexor tendon
Attaches at the medial epicondyle
Ulnar collateral ligament or UCL
Starts at the undersurface of the medial epicondyle and runs down to the sublime tubercle, which is the medial side of the coronoid process.
Common extensor tendon
Originates at the lateral epicondyle.
Lateral collateral ligament
Originates just underneath the attachment of the common extensor tendon.
Lateral ulnar collateral ligament
This is a somewhat confusing term for a tendon that also originates just underneath the common extensor tendon. It swings down behind the radial head and attaches at the area of the ulna that is called the supinator crest - see lateral view.
Biceps tendon
Attaches on the radial tuberosity.
Brachialis tendon
Attaches on the coronoid process.
Annular ligament
Attaches on the volar side of the sigmoid notch of the ulna and runs around the radial head and attaches on the dorsal side of the sigmoid notch.
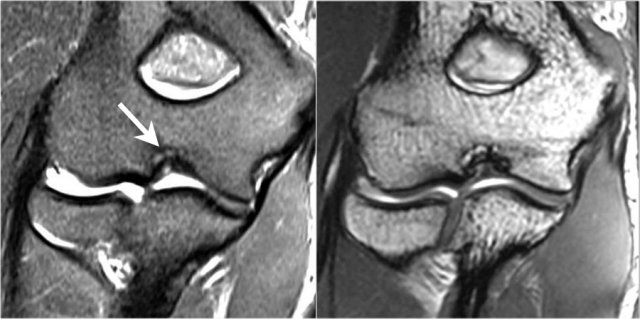
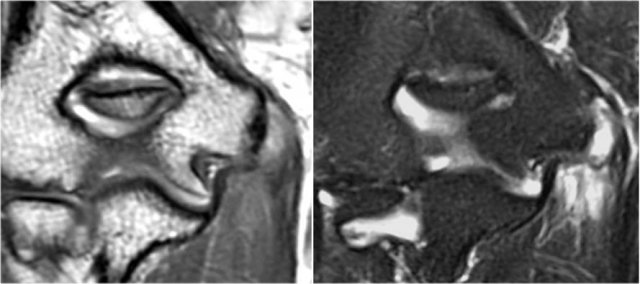
Pseudodefect of the capitellum
This is a finding that you frequently see on coronal images.
It looks like an osteochondral lesion, but if you look at the sagittal image you will notice that the coronal image runs through the posterior non-articular portion of the capitellum.
So when the elbow is fully extended, a portion of the radial head is actually behind the carticular surface of the capitellum.
On a coronal view we will be looking at the radial head which is covered with cartilage and opposite to it the non-cartilage covered part of the capitellum, which frequently is somewhat irregular.
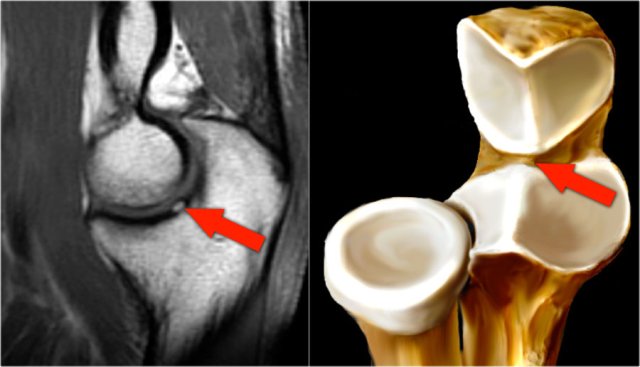
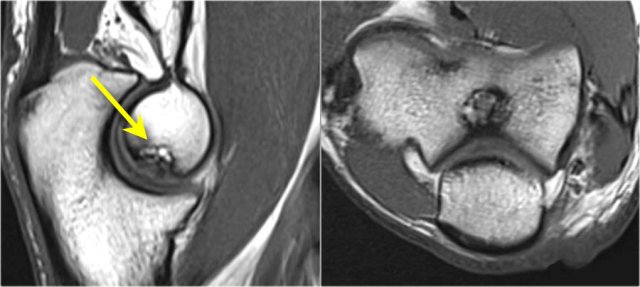
Pseudo-loose body
Another common finding is a small piece of fat that you'll see on the sagittal image, that looks like a small loose body or a cartilage defect.
This can be explained if we look at the articular surface of the olecranon.
Typically the olecranon has two pieces of cartilage with a small area inbetween, that fills with fat.
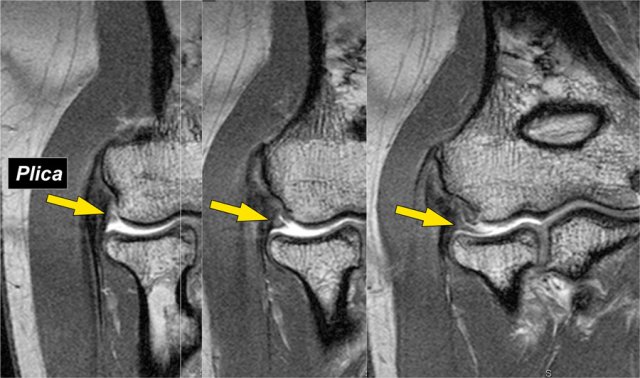
Plica
This structure on the lateral side of the joint is sometimes seen and is a plica.
It can be prominent and almost look like a meniscus.
It is a normal structure, but sometimes it is thickened or irregular and it may be a cause of symptoms.
Elbow Mechanics
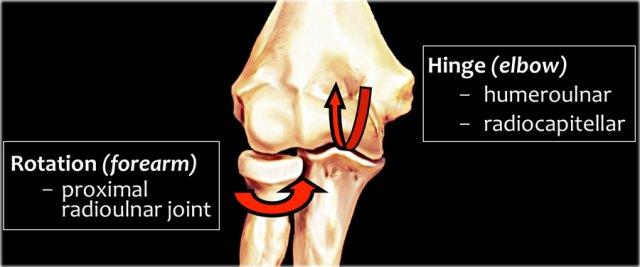
The elbow serves as a hinge joint when we look at the humeroulnar and radiocapitellar joint.
The other joint is the proximal radioulnar joint with rotation allowing pronation and supination.

Many acute and chronic injuries occur as a result of throwing.
During the throwing motion in the phase of late cocking to acceleration, there are tremendous valgus forces that are pulling the elbow.
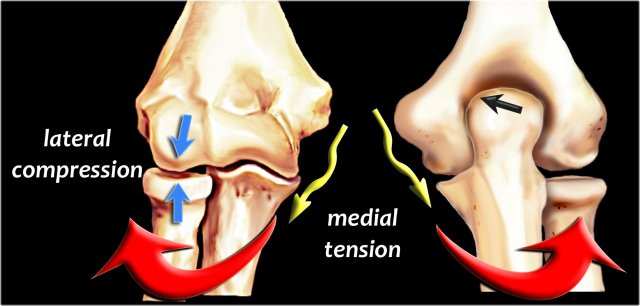
The valgus overload results in enormous tension on the medial side trying to pull things apart (yellow arrows), while the lateral side will be under compression (blue arrows).
On the posterior side it causes shear forces along the head of the olecranon (black arrow).
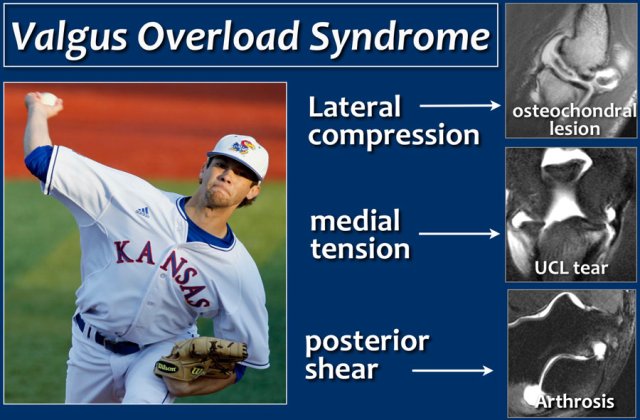
Valgus overload syndrome
All these forces make up what is called the "valgus overload syndrome" with very characteristic injuries to the elbow over time.
- The tension on the medial side causes a tear of the ulnar collateral ligament.
- Compression on the lateral side causes an osteochondral lesion of the capitellum.
- The shear forces on the posterior side cause arthrosis.
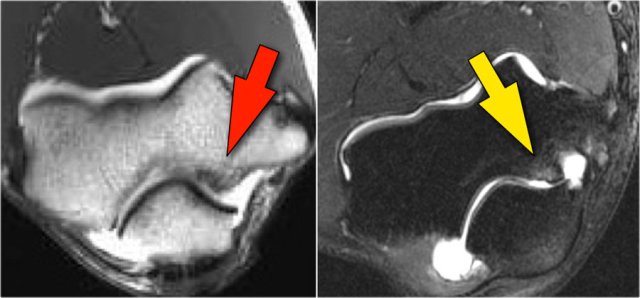
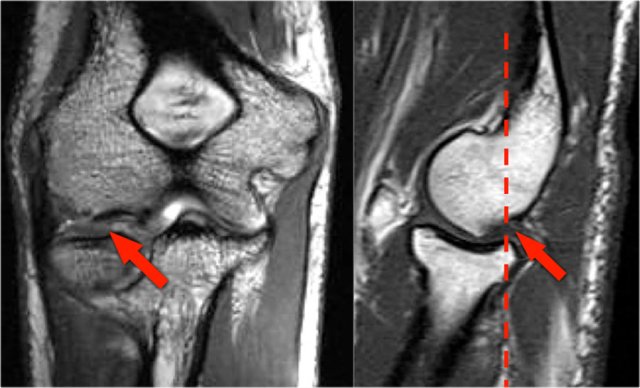
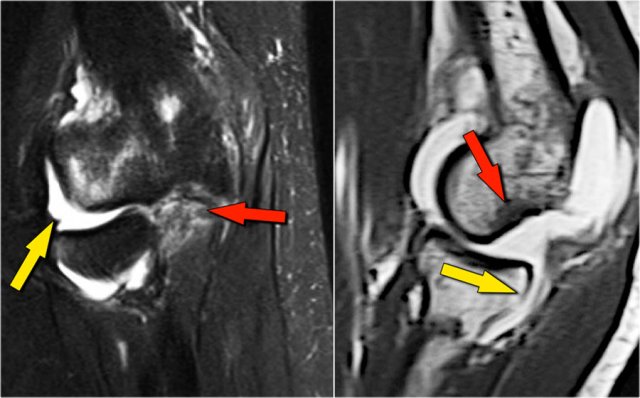
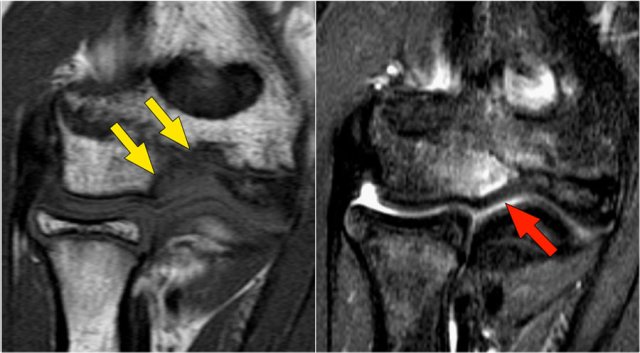
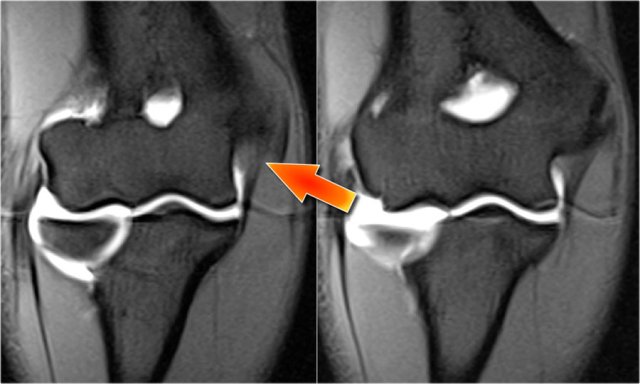
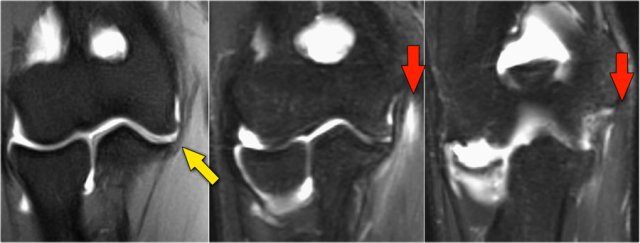
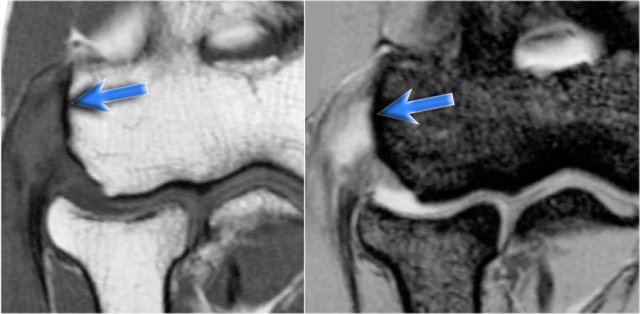
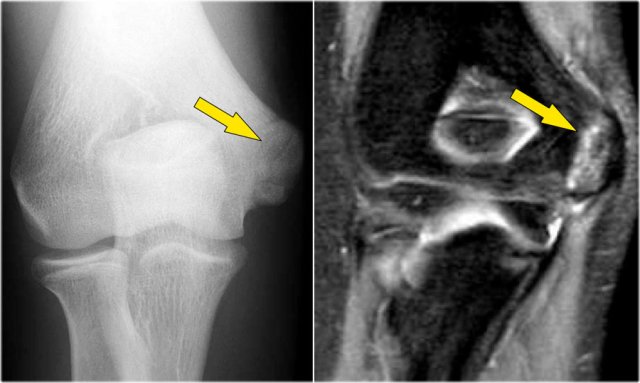
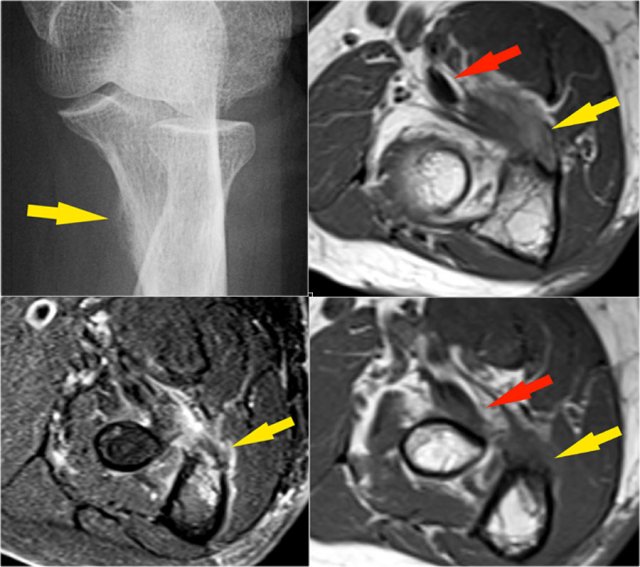
Arthrosis in valgus overload syndrome
Due to the valgus overload there are shear forces on the posteromedial part of the humeroulnar joint.
Notice the subchondral sclerosis seen on the T1W-image (red arrow).
On the T2W-image there is subchondral bone marrow edema and cartilage loss (yellow arrow).
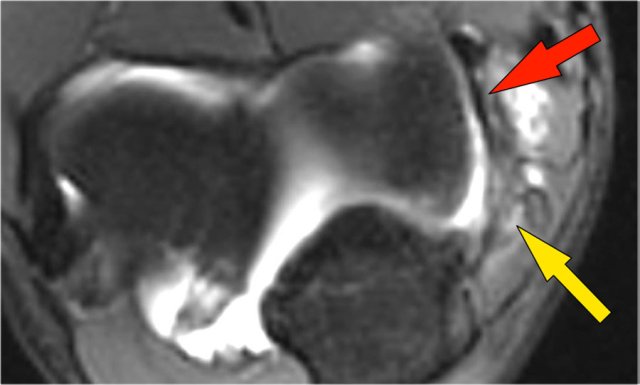
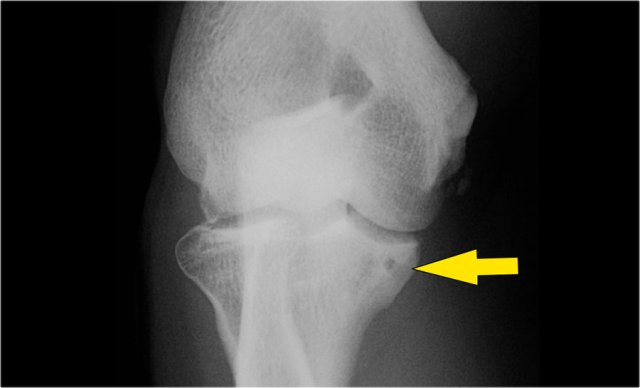
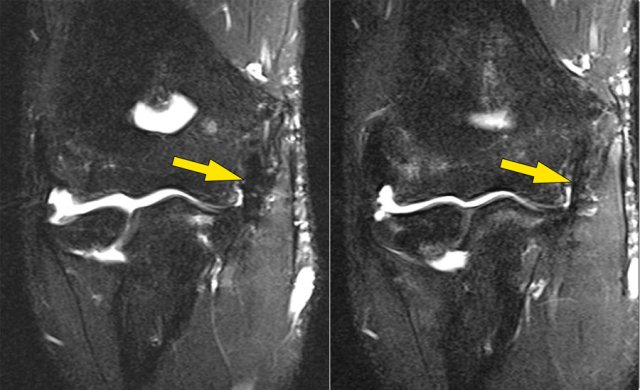
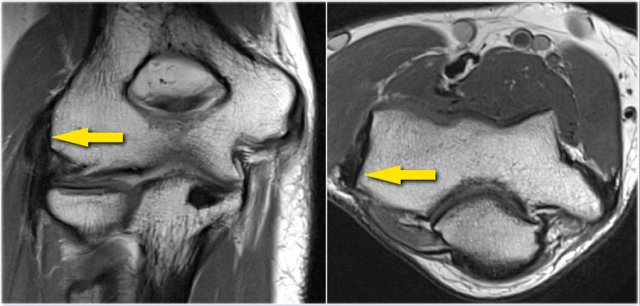
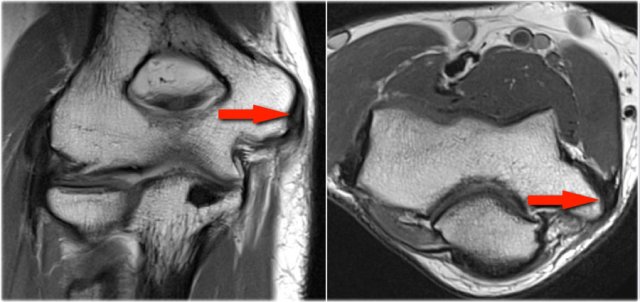
These are images of a 20 year old baseball pitcher.
Scroll through the images.
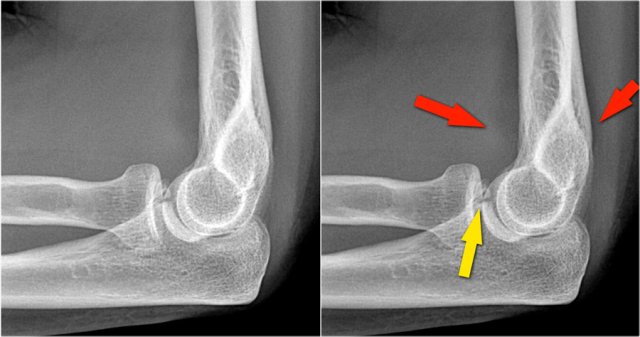
On the coronal images there is a beautiful anterior bundle of the UCL, but notice that there is osteophyte formation on the medial part of the joint (red arrow).
As we go further posteriorly there is a small area of low signal intensity (yellow arrow), which is an avulsion of part of the UCL.
This is better appreciated on the radiograph.
Continue with the axial scan.
As we look on the axial scan, we can appreciate the huge osteophyte formation.
Notice that the ulnar nerve (blue arrow) is next to these osteophytes and these patients may present with ulnar neuropathy.
Posterolateral Rotatory instability

There are different stages of instability of the elbow joint and the final stage is dislocation.
In stage 1 there is subluxation of the ulna and there is tearing of the lateral ulnar collateral ligament.
In stage 2 there is more injury, where the coronoid perches the trochlea and there is more ligamentous injury.
In stage 3 finally the coronoid ends up behind the humerus in a true dislocation and you may tear the ulnar collateral ligament, which results in a very unstable - floating - elbow.
Elbow dislocation
Here a lateral view of the elbow of a patient who fell on the outstretched arm.
The radiograph shows joint effusion (red arrows) and a coronoid fracture (yellow arrow).
Continue with the MR-images.
Now here is the MR.
Study the images and then continue reading...
Coronal view:
- Lateral collateral ligament is completely stripped (yellow arrow).
- radial head is subluxed.
- marrow edema of the coronoid process due to the fracture (red arrow).
Sagittal view:
- Radial head is a little bit subluxed posteriorly (yellow arrow).
- Large effusion and capsular disruption posteriorly.
- Contusion of the posterior side of the capitellum as a result of impaction by the coronoid process (red arrow).
All these signs are the result of a posterior dislocation.
Read more in the article of Zehava Rosenberg in AJR 2008 entitled: MRI Features of Posterior Capitellar Impaction Injuries
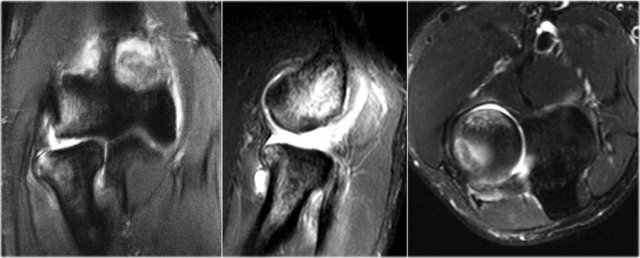
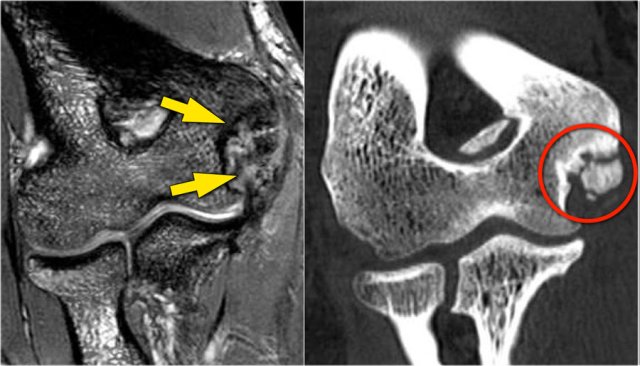
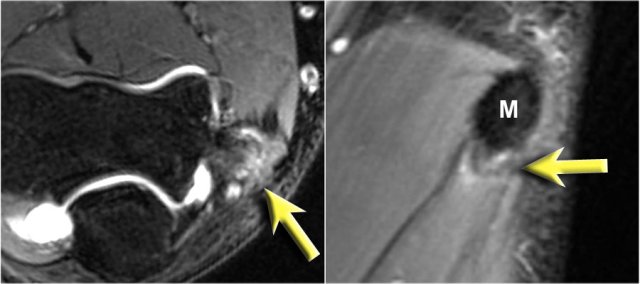
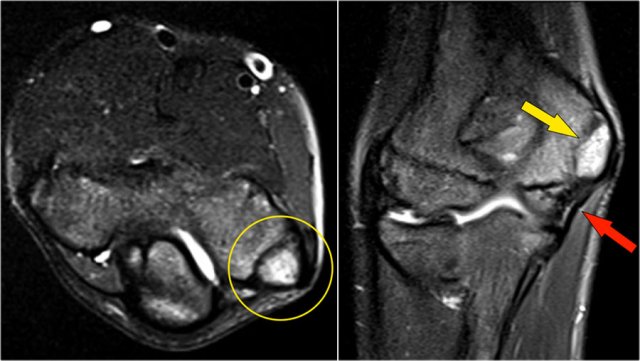
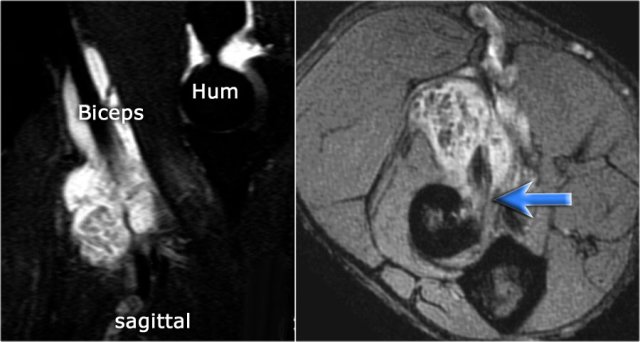
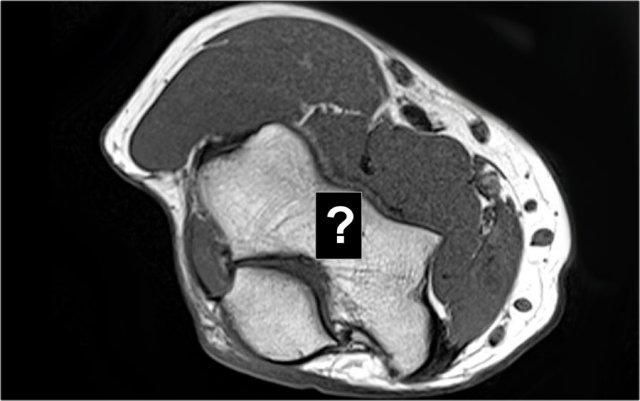
These images are of a 23 year old male who fell onto his outstretched hand two weeks ago while skateboarding.
On physical exam there was decreased range of motion of the elbow and tenderness along the lateral aspect.
First study the images, then continue reading...
What is the structure on the axial image behind the radial head?

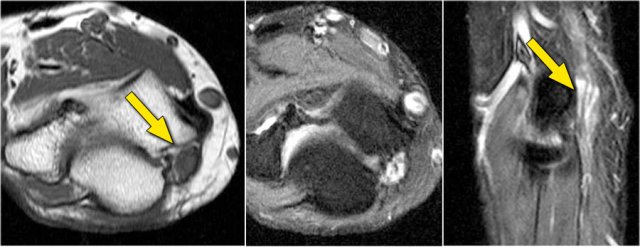
Sagittal view:
- Again the characteristic pattern of marrow edema that is seen in posterior elbow dislocation with contusion in the anterior side of the radial head (red arrow) and on the posterior side of the capitellum.
- The radial head must have hit the posterior part of the capitellum.
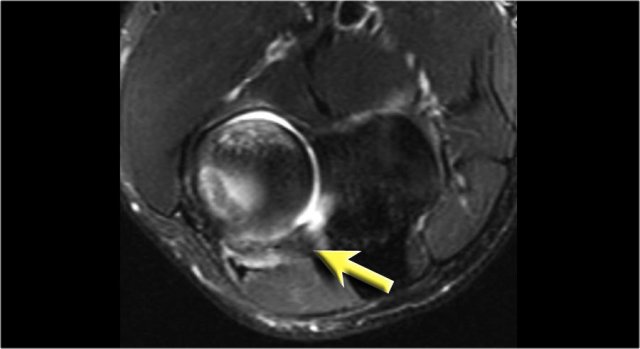
The structure behind the radial head is the annular ligament.
It is irregular and thickened as a result of the posterior dislocation.
Osteochondral lesions

OC lesion of capitellum
Osteochondral lesion is the new name for osteochondritis dissecans or OCD.
The chronic valgus overload can cause an osteochondral lesion on the lateral side of the elbow.
It is the result of repetitive impaction and shear forces.
The radiograph is of a 15 year old baseball player with 4 year history of elbow pain and a recent episode of locking.
There is a focal lucency in the capitellum and some fragmntation.
This is typical for a osteochondral lesion of the capitellum and the locking is probably the result of loose bodies.
Continue with the MR...
The MR-arthrogram confirms the osteochondral lesion.
There is gadolinium in between the humerus and the osteochondral lesion which indicates that it is unstable.
If you don't have gadolinium, look for joint fluid undercutting the fragment.
There is a loose body in the posterior recess of the radiocapittelar joint.
Notice also the fragmentation as seen on the axial image.

The osteochondral lesion of the capitellum is typically seen in throwers and gymnasts (11-15 yrs), who get a lot of wrist and elbow problems due to weight bearing.
Here another case in a 20 year old gymnast.
Again there is lucency on the radiograph.
The MR-arthrogram shows some bone marrow edema on the coronal view.
The sagittal T1W-image shows subchondral bone abnormality, but not much of a fragment.
There is some cartilage thinning, but not a defect.
This is obviously a stable fragment and there were no loose bodies.
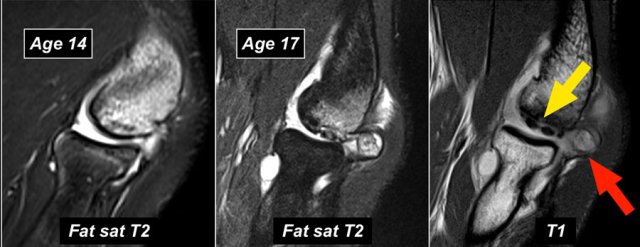
These images are of a young baseball player, who presented with elbow pain at age 14.
The T2W-fatsat image shows marrow edema and maybe there is a subchondral fracture.
Obviously someone told him to keep throwing, because he came back three years later at age 17 and you can see what can happen when they push too hard in getting these kids to become a professional.
The T1W-image shows fragmentation (yellow arrow) with a loose body (red arrow).
The T2W-image demonstrates that the fragment is unstable because there is high signal between the fragment and the humerus.
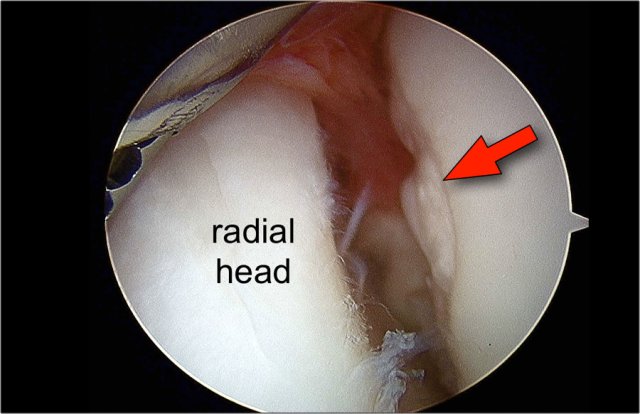
At arthroscopy there is depression and irregularity of the cartilage of the capitellum.

First the loose bodies were taken out.
Then frequently an OATS-procedure is performed, which we will discuss now.
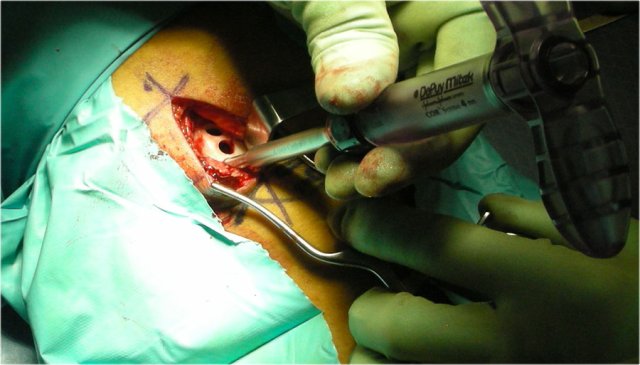
OATS procedure
OATS stands for osteochondral autologous transfer.
Pieces of cartilage and bone are taken out of some other non-weight bearing bone and tranferrred to the capitellum.
In this patient the cartilage is taken from the non-weight bearing part of the knee.
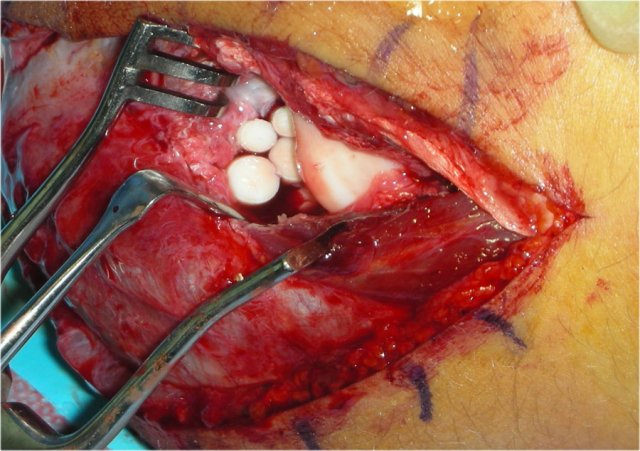
Then holes are drilled in the capitellum and the defects are filled with the autologous bone and cartilage.
Here the hole in the capitellum is filled with four pieces of bone and cartilage.
The radial head is seen opposite the capitellum.
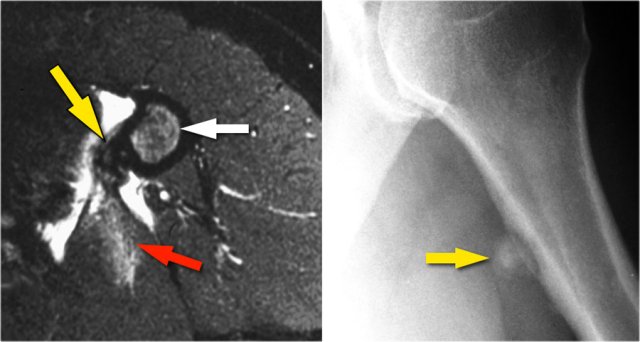
OC lesion of trochlea
These images are of a patient with anterior elbow pain.
There was no recent injury.
The clinical diagnosis was a biceps tendinitis or a bicipital bursitis.
The findings on the coronal MR-images are quite uncommon.
If you would see this in the capitellum you would call it an osteochondral lesion of the capitellum.
So this is called an osteochondral lesion of the trochlea.
Notice the small cystic changes (white arrow).
There is also a small cartilage defect.
An osteochondral lesion of the trochlea is usually seen in younger patients, who have an immature skeleton.
It is seen in the lateral trochlea like in this case due to repetitive hyperextension in an area with tenuous blood supply.
It is also seen in the medial trochlea due to laxity and posteromedial abutment.
Here a different patient.
Notice that it is a young patient, because the physis is still open.
There is a large osteochondral lesion in the lateral trochlea (yellow arrows).
Notice the edema in the subchondral bone (red arrow).
The cartilage is still intact.
Ulnar Collateral Ligament
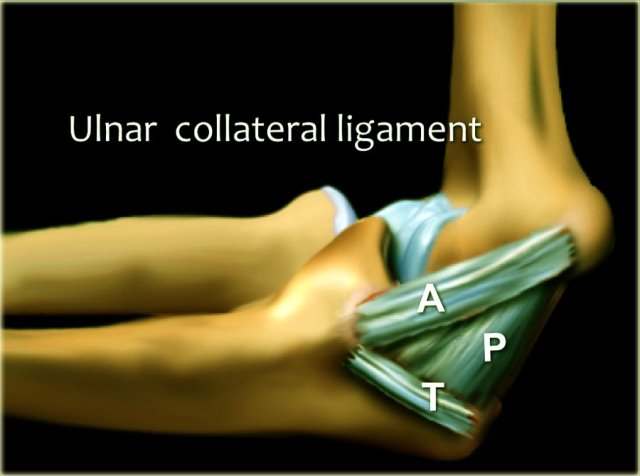
The ulnar collateral ligament (UCL) is situated on the medial side and it has three components.
The anterior bundle is the strongest component and is the primary restraint against valgus forces.
On MR this is the most important structure.
The posterior bundle attaches distally in a fan-shape on the olecranon.
It forms the floor of the cubital tunnel.
The transverse bundle runs from the olecranon to the olecranon, so it doesn't do much.
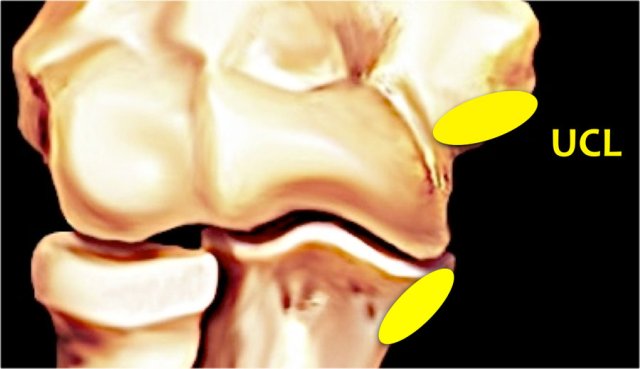
The UCL (in yellow) originates on the undersurface of the medial epicondyle just beneath the origin of the common flexor tendon.
It attaches on a small process on the medial side of the coronoid, which is called the sublime tubercle.
Always use the axial images when you study the ligaments, especially the UCL.
Scroll through the images.
- If you look at the medial epicondyle you will notice the posterior bundle as a thin structure (blue arrow).
- Notice the ulnar nerve sitting in the cubital tunnel.
- The posterior bundle forms the floor of the cubital tunnel.
- A retinaculum covers the cubital tunnel.
- Notice that the anterior bundle is much thicker (white arrow).
- You can see the difference between the anterior and posterior ligament even though they form one ligament.
- As we go distally we'll see that they merge together to attach to the sublime tubercle.
 text
text
Here we see two consecutive coronal images of the UCL.
It is normal to see some high signal in the proximal part (arrow).
Notice how it firmly attaches to the sublime tubercle and compare this to the next images.
 text
text
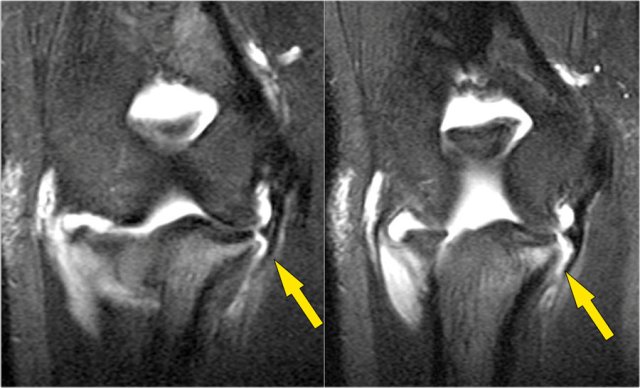
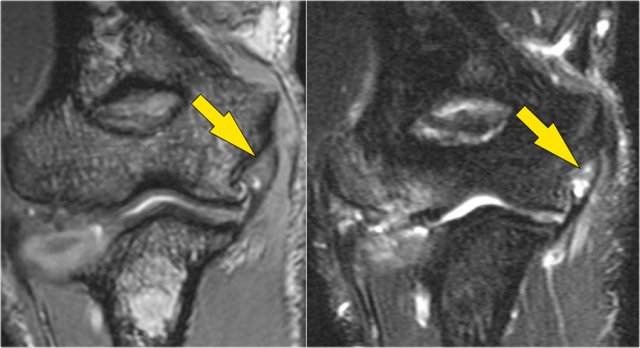
UCL tear
Remember that the UCL should attach very tightly on the sublime tubercle.
In this case it doesn't, so even on these two images you can tell that there is a complete tear.
Notice that there is some marrow edema in the sublime tubercle.
The mechanism of injury to the UCL is usually chronic tensile forces, which create microtears.
This is seen in pitchers and other overhead throwing-athletes.
A tear can also occur in a fall on the outstretched hand.
Most commonly there is a complete tear, but sometimes there is a partial tear which can be very hard to see.
That is why in these athletes MR-arthrogram is usually performed.
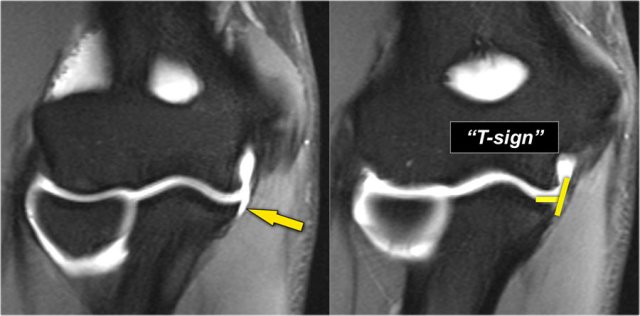
Study the images and then continue reading...
This is a 18 year old baseball pitcher with medial elbow pain.
A partial tear is seen creating a 'T-sign'.
First study the coronal T2-fatsat images and then continue reading...
Notice that the anterior bundle is intact and firmly attaches to the sublime tubercle (yellow arrow).
On the next two images there is some soft tissue edema and more abnormal signal posteriorly (red arrow). So we suspect pathology of the posterior bundle.
Now you remember that the axial images can be helpful.
So continue with the axial image.
On the axial image we nicely see the anterior bundle is o.k. (red arrow).
There is only some edema next to it.
However the posterior bundle is not o.k.
This is partial tearing.
We see this occasionally in throwing athletes, where the anterior bundle is intact and their elbow is not unstable.
They somehow have torn their posterior bundle, which causes pain.
They do not need surgery, but it still may keep them out of the game for quite a while.
Now here is the last case.
This is a 38 year old male who has been weight-lifting for 20 years.
He complains of intermittent elbow pain and popping.
Notice that the UCL is abnormal with some areas of very high signal indicating a partial tear.
On the lateral side there is subchondral edema and cartilage loss.
This is arthrosis secondary to chronic instability due to the chronic partial tearing.
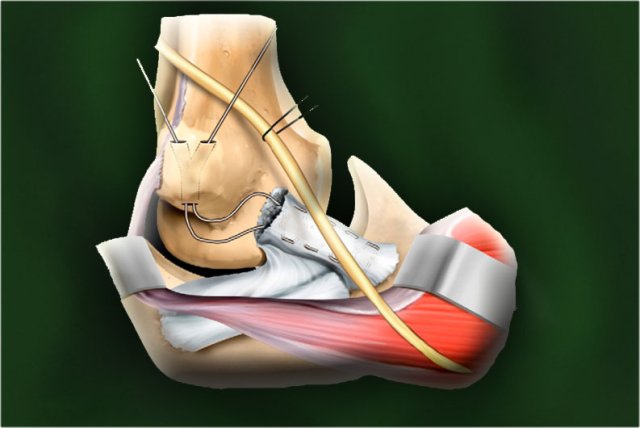
UCL repair
UCL repair is done by placing tunnels in the medial epicondyle.
They run done to the sublime tubercle and a graft is placed in between them.
This radiograph is of a 26 year old professional baseball player who had a UCL reconstruction.
Notice the tunnels (arrow).
This operation usually works very well.
If you scroll through the MR-images you can see the tunnel in the medial epicondyle.
Just like in an ACL-graft we can see the low signal of the graft going all the way down.
On the coronal images despite the spiky artifacts it almost looks like a normal UCL.
Here we see images of a patient after repair who did not do so well.
There is fragmentation of the bone and disruption of the graft.
On the CT-scan it is better appreciated that there is a fracture through the tunnel.
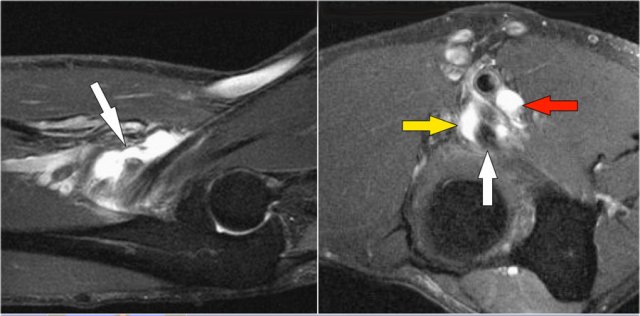
Lateral Collateral Ligament

Here an illustration of the lateral collateral ligament complex.
It consists of the radial collateral, the lateral ulnar collateral and the annular ligament.
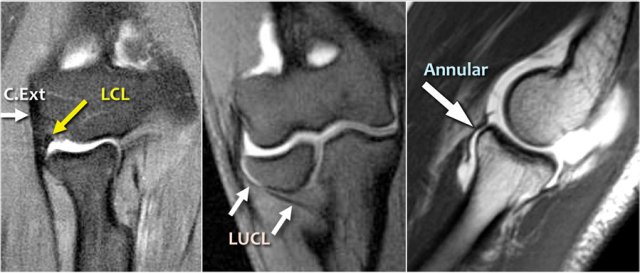
When you look for the radial collateral ligament, first try to identify the common extensor tendon, because right underneath it you will find the radial collateral ligament (yellow arrow).
As you go more posteriorly you will see the LUCL - the lateral ulnar collateral ligament, which sweeps behind the radial head (white arrows).
The annular ligament is usually difficult to differentiate from the RCL, but sometimes it can be identified on a sagittal MR-artrogram.
Scroll through these images.
You can also enlarge them.
Common Extensor Tendon
The common extensor tendon originates at the lateral epicondyle.
On a T1W-images the tendon should have a low signal intensity (yellow arrow).

Lateral Epicondylitis
Lateral epicondylitis is also known as the tennis elbow, although in 95% of cases it is seen in non-tennis players.
It is due of chronic stress to the common extensor tendon, which results in partial tearing and tendinosis.
Typically, the extensor carpi radialis brevis is the component that is involved.
In more severe cases there is tearing of the LCL, which gives a poor response to conservative treatment.
Here a typical case.
There is thickening and abnormal intrinsic signal on both T1- and T2W-images.
Common Flexor Tendon
The common flexor tendon originates at the medial epicondyle.
On a T1W-images the tendon should have a low signal intensity (red arrow).
Medial Epicondylitis
This is the counterpart of the lateral epicondylitis and also known as the golfer's elbow.
Here the common flexor tendon is involved.
On the sagittal image it is clear that it is only partial tearing.
However this can be quite painful.
Here we have the coronal T1W- and T2W-images.
There is partial tearing, but it is very extensive.
Little Leaguer's Elbow
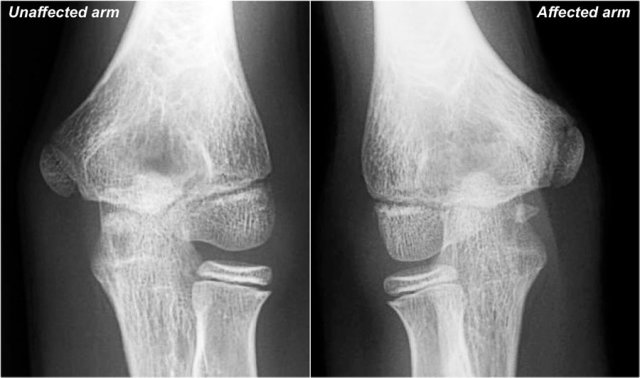
First study the images of a patient with pain on the medial side, then continue reading...
The findings are very subtle.
The medial epicondyle of the affected arm is somewhat more osteopenic.
In these cases we usually ask for a comparison view, because it can be very subtle.
The diagnosis is a Little leaguer's elbow which results from chronic stress injury.
The lucency on the radiograph, which looks like a widened physis, is due to cartilage ingrowth in the metaphysis.
Continue with the MR...
On the MR the abnormality is very obvious.
There is marrow edema in the medial epicondyle and also in the adjacent bone (yellow arrow).
Little Leaguer's elbow is also known as medial apophysitis and some call it epiphysiolysis.
By the way this could also be called a Salter-Harris type I fracture, if it was an acute traumatic event.
Notice the normal ulnar collateral ligament (red arrow).
In children the weak link in valgus stress is not the ulnar collateral ligament but the physis.
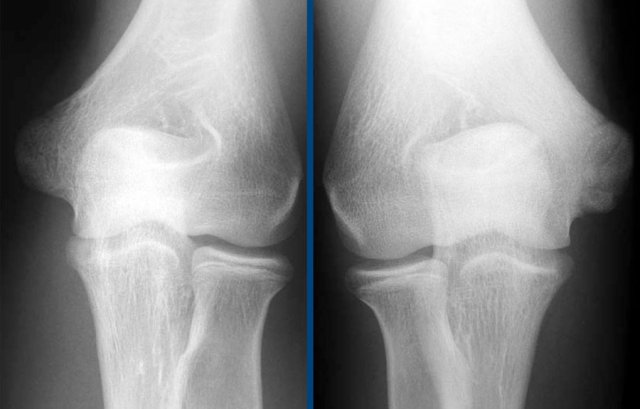
Here another case.
This patient is a little bit older.
The left epicondyle is already fused, but on the right the physis is still a little bit open.
Continue with the MR...
On the MR there is marrow edema.
Notice that there is also some edema where the ulnar collateral ligament attaches, so there is also some tearing of the UCL.

Here some more views of a different patient.
Biceps tendon
Scroll through the axial images of the biceps tendon from the musculotendinous junction to the attachment on the radial tuberositas.
The pathology of the distal biceps tendon is much like pathology in the achilles tendon.
There can be tendinosis, partial tear and complete tear with or without retraction.
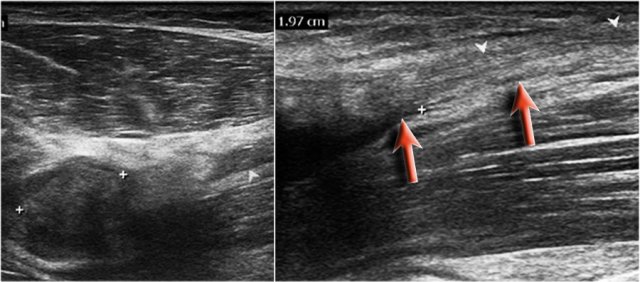
Here are the ultrasound images of a 73 year old male who experienced a sudden pain and a tearing sensation when lifting a box.
There was pain with pronation and supination and tenderness anteriorly proximal to the elbow joint.
No ecchymosis or palpable mass.
On the sagittal image the tendon is thickened, but distally the tendon is lost.
MRI examination was performed.
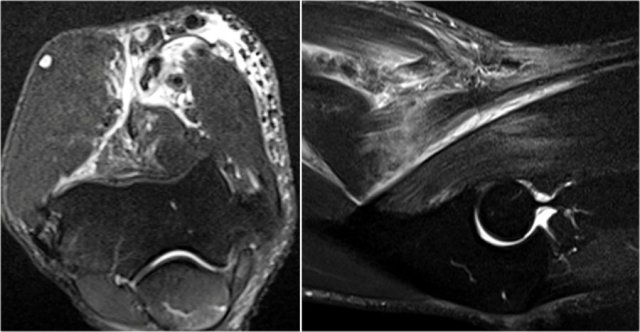
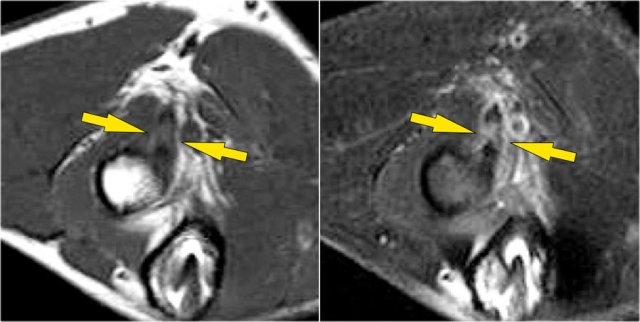
Now look at the MR-images and try to figure out if the tendon is retracted and whether there is a partial or complete tear...
Well on the sagittal image it looks as if the tendon is completely thorn, but continue with the next images.
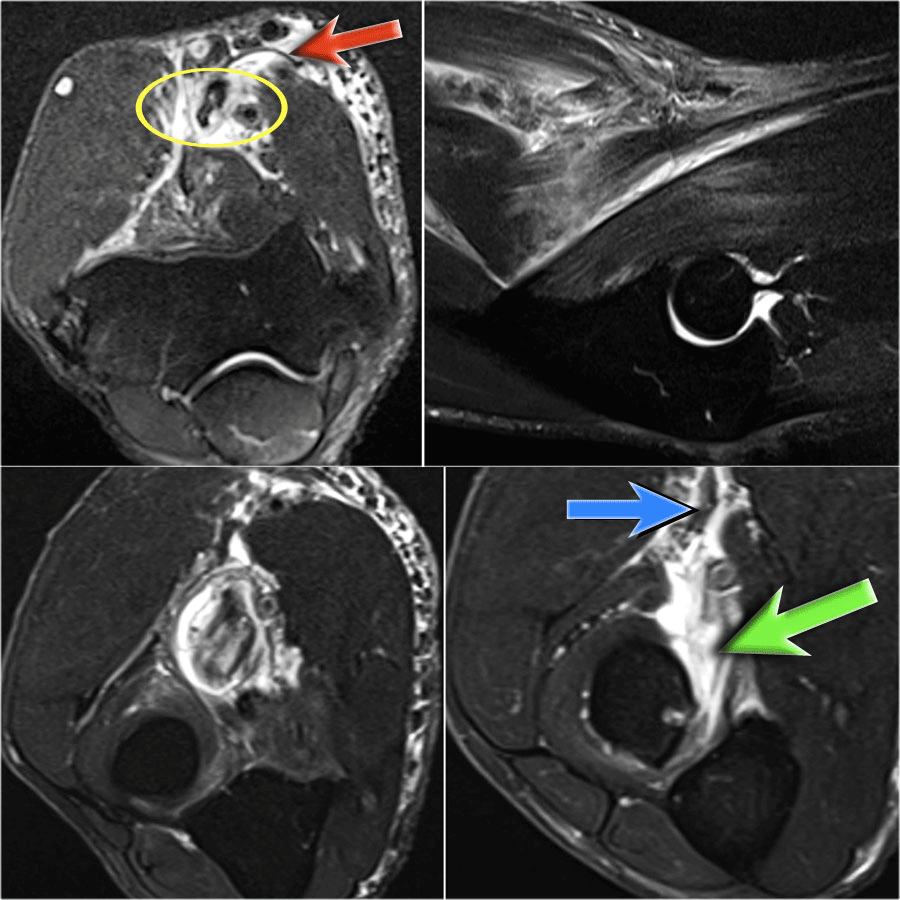
Tear of distal biceps tendon
There is a complete tear, because if we follow the tendon all the way to the radial tuberosity, we can see that the tendon does not attach there (green arrow).
There is only fluid.
The reason why the tendon is not retracted is because the broad bicipital aponeurosis - also known as lacertus fibrosus - is still intact (red arrow).
The distal biceps tendon not only inserts to the radial tuberosity, but also via the lacertus fibrosus into the fascia of the flexor pronator mass on the medial side of the forearm.
The distal tendon of the biceps is encircled on the upper left image.
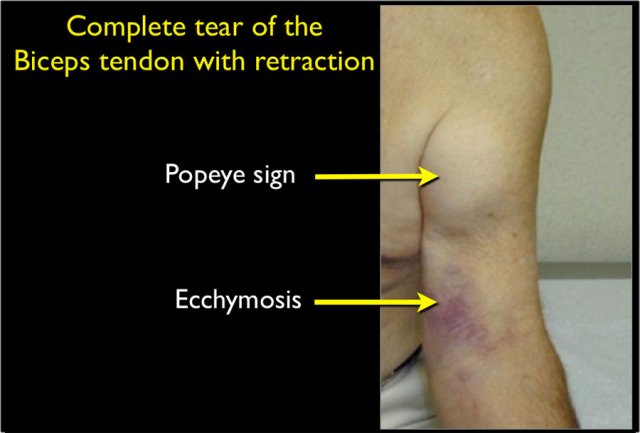
When the aponeurosis is also thorn, then the tendon retracts and you get an obvious swelling in the arm caused by the contracted biceps muscle.
A distal biceps tendon tear is an uncommon injury.
It is seen in about 5% of biceps injuries.
It is the result of a sudden extension force to the arm when the elbow is flexed.
A proximal biceps tendon tear is more common.
Usually it is the long head of the biceps that is completely torn.
Here another example.
On the T1W-image there is some thickening and some intermediate signal.
This could be tendinosis, but always look at the T2W-images to look for a tear.
In this case there is a partial tear.
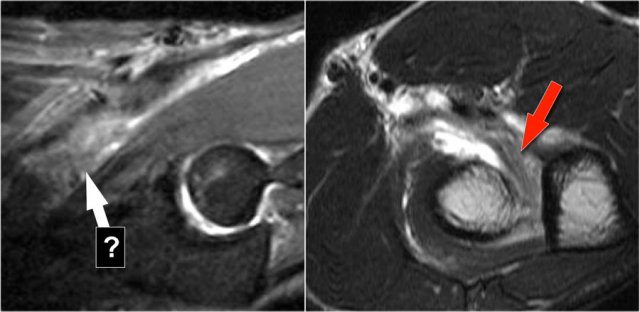
Here another case.
On the sagittal images we were not sure about a possible tear.
Maybe there only was some tendinosis or tendinitis.
The axial images demonstrate a high grade partial tear (red arrow).
Always make sure that your axial scan goes all the way to the tuberosity, because is you stop too early, like in this case, then you will only see a thickened tendon and some fluid, but you are not sure about a possible tear.
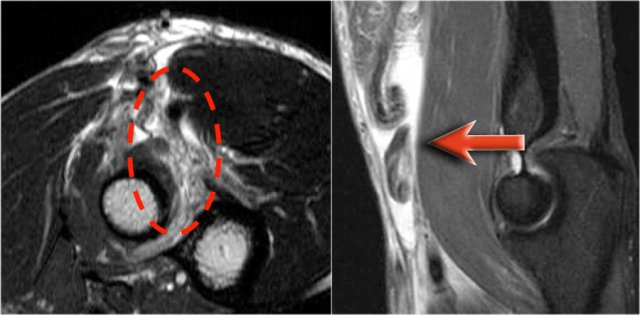
Here an easy case, because the tendon is retracted as can be best seen on the sagittal image.
So the lacertus must also have been torn.
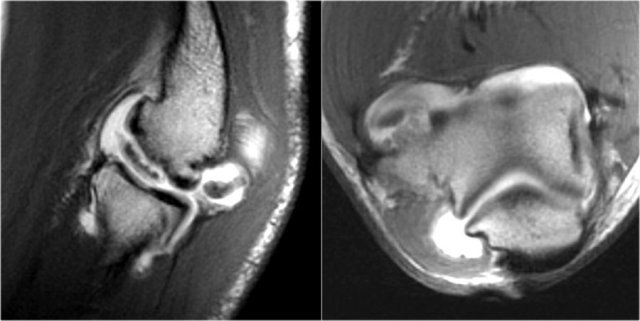
Radiobicipital bursitis
Here are sagittal and axial images of a patient who was referred to an orthopedic oncology surgeon for a mass near the elbow.
There is a partial tear (arrow) of the biceps tendon, but the question is, what is the structure that we are looking at and what is within it.
The structure is the radiobicipital bursa, so this is a bursitis.
Remember that the biceps tendon does not have a tendon sheaht, so tenosynovitis is not a possibility.
The differential diagnosis for the low intensity structures within the bursa is: synovial chondromatosis, PVNS and rice bodies.
It turned out to be rice bodies.
In any synovial lined joint or bursa these rice bodies can be formed as a result of chronic inflammation with synovial hypertrophy.
The villi will outgrow their blood supply, become necrotic and fall into the joint or bursa.
They are called rice bodies because when you open up the joint, they just look like rice.
Here another case.
The white arrow in the left sided image is pointing to the bursa.
Notice that the biceps is intact.
Next to the radiobicipital bursa (yellow arrow), also an interosseous bursa (red arrow) was described by Abdalla Skaf in Radiology in the article entitled: Bicipitoradial Bursitis: MR Imaging Findings.
Sometimes these masses mimic a tumor or they can cause impingement on the radial nerve when they become very large.
Brachialis tendon
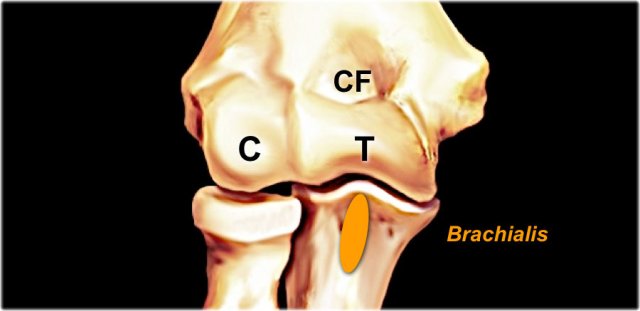
The brachialis originates from the lower half of the front of the humerus, near the insertion of the deltoid muscle.
It lies deeper than the biceps brachii, and is a synergist that assists the biceps in flexing the elbow.
The thick tendon inserts on the anterior surface of the coronoid process of the ulna.

On a sagittal view, when you compare the brachialis tendon (yellow arrows) with the biceps tendon (red arrows), notice that the brachialis is almost all muscle.
It only has a very short tendon distally.

Chronic avulsion
This image is of a 68 year old woman who injured her arm approximately 10 years previously and now presents with increasing pain in that arm.
First study the radiograph and then continue with the MR...
First study these axial T1W-images and then continue reading...
Radiograph
The cortex of the ulna is irregular and in a 68 year old woman there was concern of underlying bone abnormality like for instance a bone tumor.
MRI
The biceps tendon is indicated by the red arrow and demonstrates tendinosis and partial tearing.
However when we look at the insertion of the brachialis tendon on the coronoid process, there is tearing of the tendon with a lot of bone marrow edema as seen on the fat suppressed T2W-image.
In fact this was a chronic type of avulsion injury with partial tearing of the tendon.
The bone reaction can mimic an aggressive bone lesion.
Here another chronic avulson, which was sent to the oncologic surgeon, because there was concern about a possible juxta-cortical osteosarcoma.
The MR however revealed the following:
- The lesion was located at the insertion of a latissimus dorsi tendon to the humerus (yellow arrow).
- The bone marrow has a little bit of high signal, but otherwise does not look that abnormal.
- There is also injury to the muscle aswell (red arrow).
Chronic avulsive injuries are common in adolescents, but may also be seen in older patients.
The problem is that they may mimic infection or tumor.
Nerves
Scroll through the images.
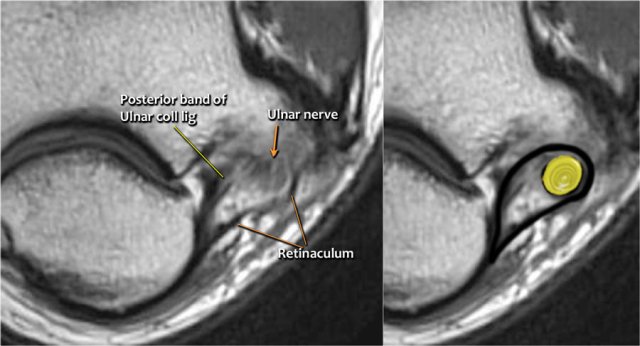
Ulnar nerve
Here we see the ulnar nerve within the cubital tunnel.
The posterior band of the ulnar collateral band forms the floor of the tunnel, while the retinaculum forms the roof.
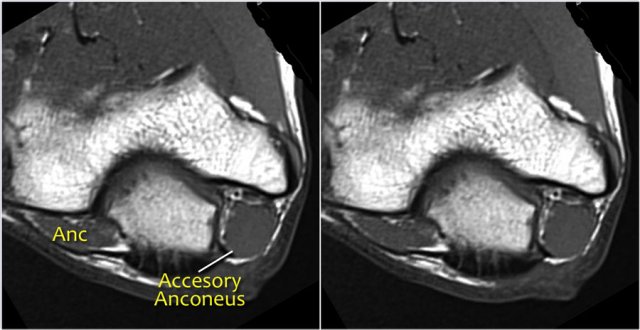
First study the images.
This patient had ulnar nerve neuropathy.
What is the cause?
Cubital tunnel syndrome is a common peripheral neuropathy.
It arises from compression of the ulnar nerve within the cubital tunnel, where the nerve passes beneath the cubital tunnel retinaculum.
Possible causes of cubital tunnel syndrome:
- Overuse
- Subluxation of the ulnar nerve because of congenital laxity in the fibrous tissue
- Humeral fracture with loose bodies or callus formation
- Arthritic spur arising from the epicondyle or olecranon,
- Muscle anomaly (eg, an accessory anconeus muscle) as is present in this case.
- Soft-tissue mass: ganglion, lipoma, osteochondroma, synovitis secondary to rheumatoid arthritis, infection (eg, tuberculosis), and hemorrhage.
Read more on neuropathy in the 2006 Radiographics article by Gustav Andreisek et al entitled:
Peripheral neuropathies of the median, radial and ulnar nerves: MR imaging features.
What is missing in this image and what is the probable cause...
The ulnar nerve is not where it is supposed to be.
Now the nerve could be dislocated, but in this case the nerve was surgically transposed.
Ulnar nerve transposition is performed in patients in whom the ulnar nerve is compressed against the medial epicondyle.

So the question is, when they take the ulnar nerve out of the tunnel, where do they put it.
This can be subcutaneous, submuscular or intramuscular.
So when we go back to the image, you will notice that it can be difficult to find the nerve.
Any of these subcutaneous structures could be the transposed nerve.
A way to do it, is to follow the structures distally until you find the ulnar nerve distally in its normal position in the proximal forearm surrounded by fat.
Then when you follow it proximally, you will notice that this was a subcutaneous transposition.
In this case, there is neuritis.
There is enlargement of the nerve.
On the T2W-image there is high signal.
Another sign is non-uniform enlargement of the fascicles, which is seen on the sagittal image (arrow).
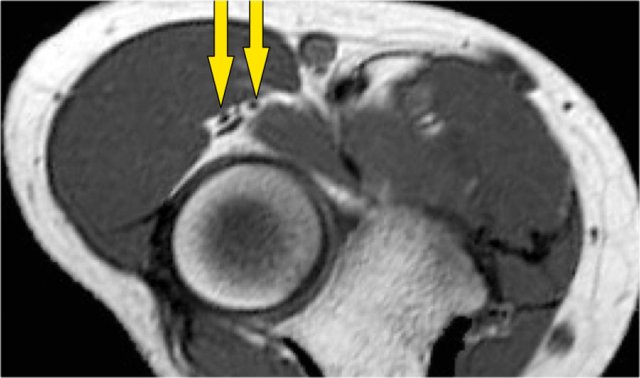
Radial nerve
The radial nerve can be best identified at the level of the radial head, where you can see superficial and deep branches in the radial tunnel (arrows).
This is a very consistent place to find the radial nerve.
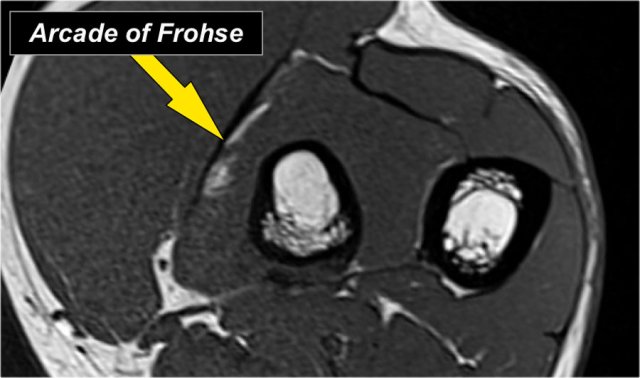
The deep radial branches form the posterior interosseus nerve which penetrates the supinator muscle at the arcade of Frohse (arrow).
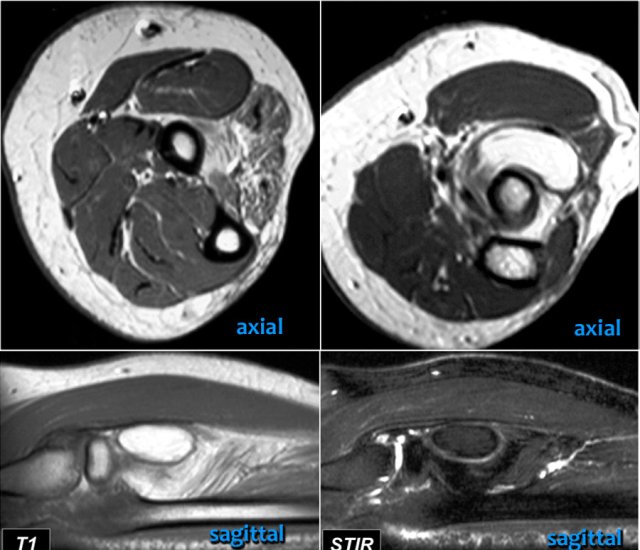
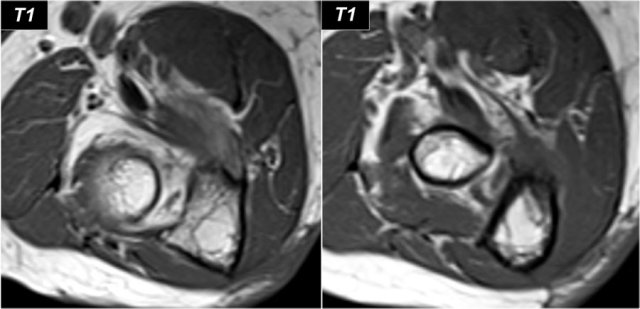
Study these images and then continue reading.
What are the findings?
The findings are:
- On the upper left T1W-image there is high signal fat within the extensor muscles with loss of muscle bulk which indicates fatty atrophy.
- The axial image on the upper right shows a mass more proximally in the supinator muscle.
- The sagittal images confirm that this is a lipoma.
So the atrophy is a result of compression of the posterior interosseous nerve, which is a branch of the radial nerve.
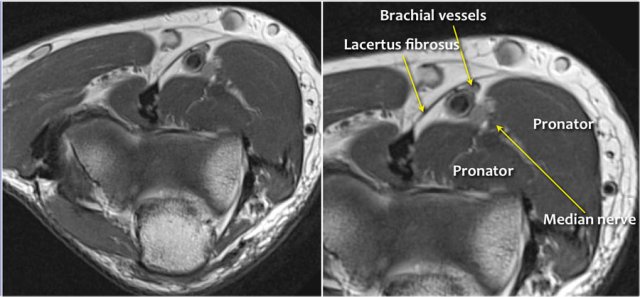
Median nerve
The median nerve goes down behind the Lacertus fibrosis, which is the aponeurosis of the biceps and penetrates the pronator muscle.
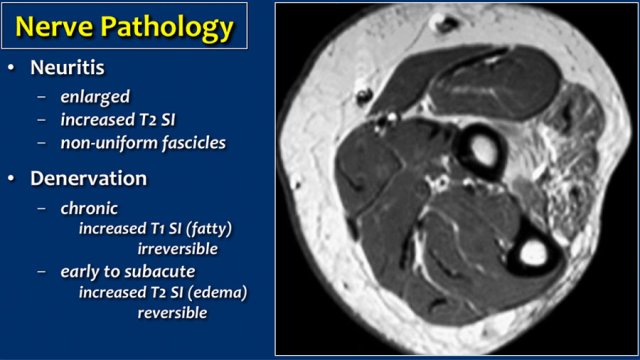
Denervation
Nerve pathology can present as thickening of the nerve when there is neuritis or as a result of compression of the nerve.
A secondary sign of nerve pathology is denervationwith edema and/or atrophy of the muscle.
In this case there is chronic atrophy with high sinal on T1, which is irreversible.
In early or subacute denervation the prominent sign is edema with high signal on T2W-images and that is reversible.
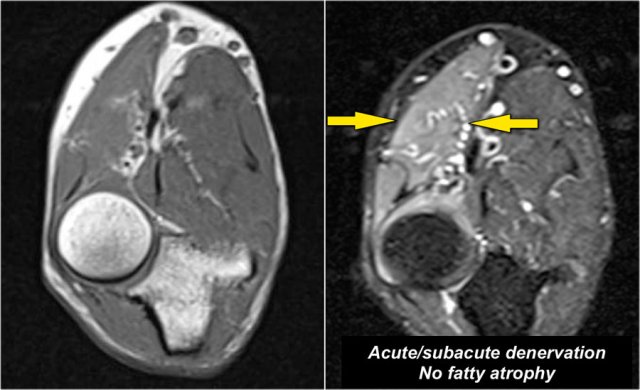
This is a 48 year old male with Marfan's syndrome, who had a sudden onset of right hand weakness.
This is a nice example of subacute denervation.
Notice on the T1W-image that there is no atrophy.
Only edema on the T2W-image.
This was due to proximal radial neuropathy.
Soft Tissue Masses

Around the elbow all kind of soft tissue masses can occur, which are also seen in other places.
If you cannot make a specific diagnosis, just call the mass indeterminate an do a biopsy, because in many cases you cannot tell the diagnosis.
The image shows an oval lesion, which just looks like a schwannoma, because it is elongated and it looks as if it follows the nerve, but it turned out to be a synovial sarcoma in an 11 year old boy.
Only make a diagnosis when you are sure of a specific diagnosis like bursitis, AVM, lipoma, PVNS or a cyst or hematoma.
 Cat scratch disease
Cat scratch disease
Here a 37 year old male who presented to the emergency department with pain, swelling and a mass at the left elbow that had been increasing over the last 3 weeks.
On MR a mass was seen just above the medial epicondyle, where the epitrochlear lymph nodes live.
The mass is very heterogeneous as is the enhancement.
Based on the MR-findings you still have to call this mass indeterminate.
The final diagnosis was cat scratch disease based on high Bartonella henselae titers.
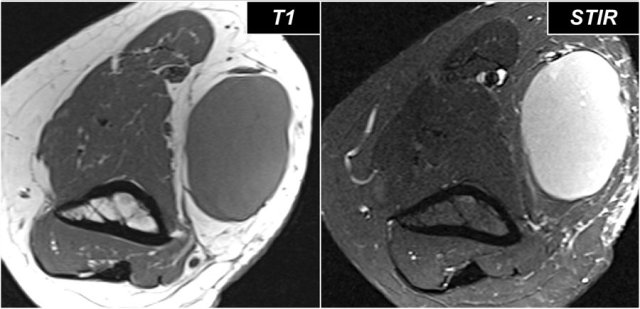
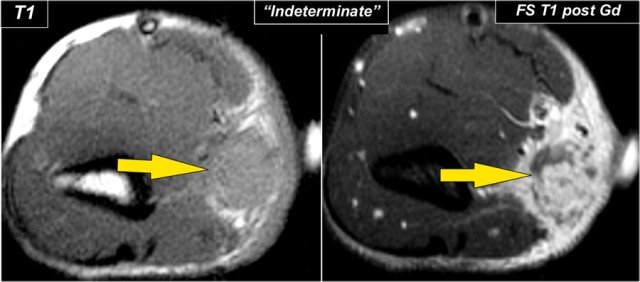
Here images of a 26 year old female who also came with a mass in the peritrochlear region.
It looks quite homogeneous and cystic.
Continue with the post-Gd image.
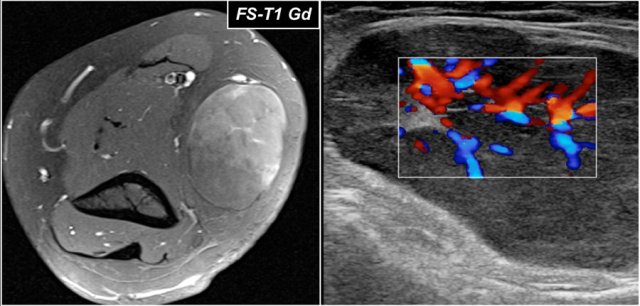
Notice the inhomogeneous enhancement on the MRI and prominent internal vascularity on the sagittal ultrasound image.
So this was not a cystic mass.
Again this was diagnosed as indeterminate.
The final diagnosis at biopsy was Lymphoma.
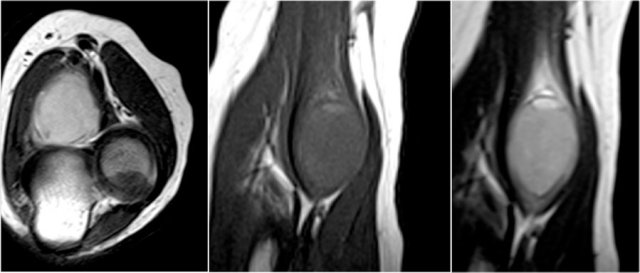
Here some additional images of the nerve-sheath tumor look-a-like, which turned out to be a synovial sarcoma.