Femoroacetabular impingement syndrome
Loes Schiphouwer¹, Adam Weir² and Robin Smithuis³
¹ Haaglanden Medical Center The Hague, ² Erasmus Medical Center Rotterdam and ³ Alrijne hospital in Leiden, the Netherlands
Femoroacetabular
(FAI) impingement syndrome is a
condition characterized by abnormal contact between the femoral head and the
acetabulum, resulting in labral and cartilage damage and causing hip pain,
particularly in young, active individuals.
FAI is also associated with early onset of osteoarthritis.
The term femoroacetabular impingement syndrome should only be applied to patients with a clinical disorder defined by the triad of:
- Symptoms in young individuals
- Clinical signs at physical examination
- Characteristic radiological findings
This article will focus on the imaging findings associated with FAI.
Introduction
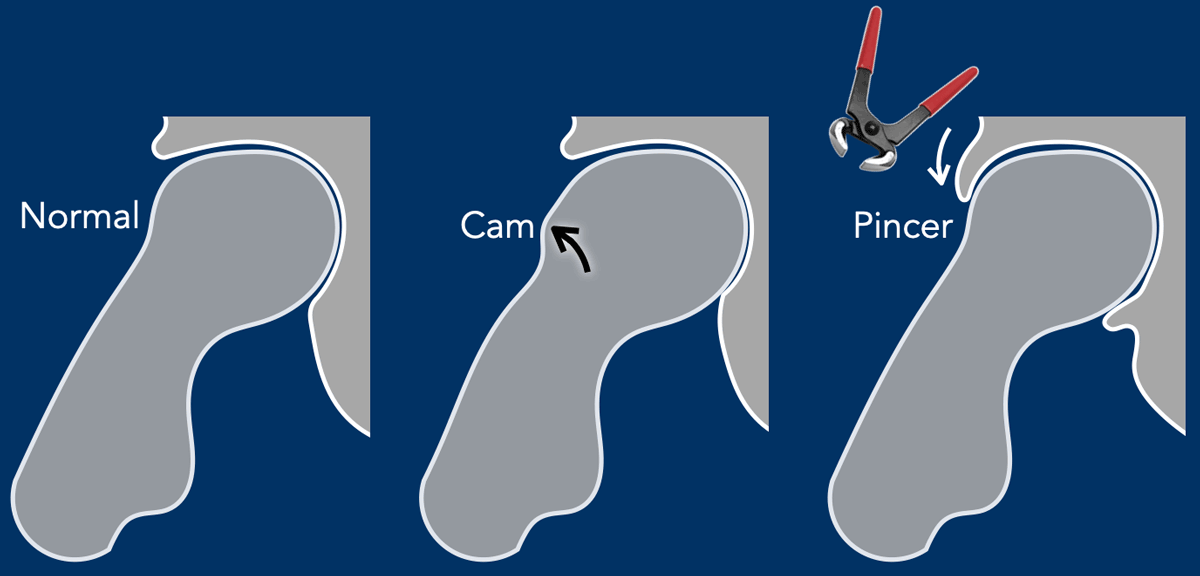
The hip joint is a ball-and-socket joint.
The femoral head, covered with cartilage, serves as the "ball" of the hip joint, while the acetabulum, deepened by the cartilage rim and labrum, functions as the "socket."
Under normal conditions, there is perfect alignment during all types of hip movements.
However, this alignment can be disrupted by bony overgrowth on the femoral side (Cam morphology) or by excessive extension of the acetabulum over the femoral head, resulting in excessive coverage of the femoral ball (Pincer morphology).
Cam and Pincer video
This video demonstrates how Cam and Pincer morphologies can lead to hip impingement.
In this video, only the osseous structures are depicted. However, it is important to understand that impingement also affects the labrum and cartilage rim, potentially resulting in labral tears and focal cartilage loss.
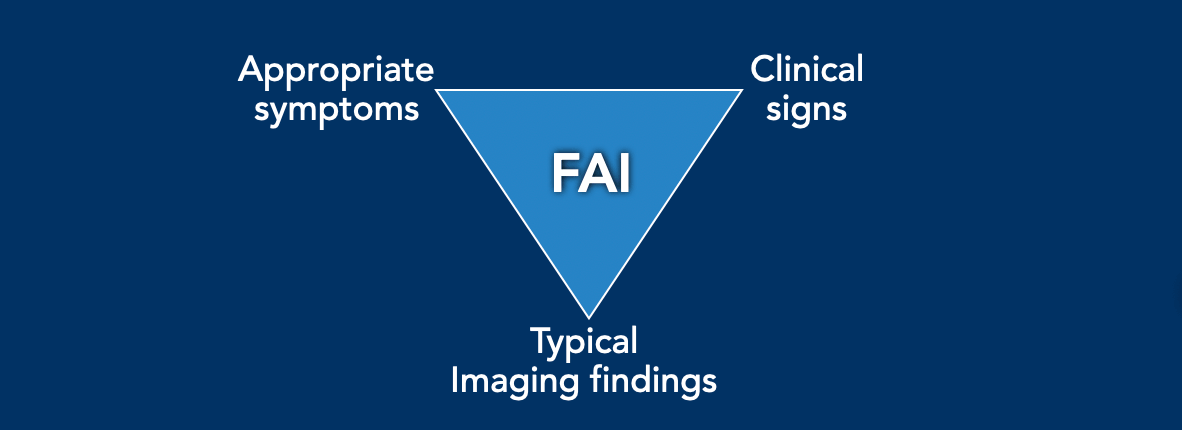
It is important to realize, that in order to make the diagnosis of femoroacetabular impingement (FAI) syndrome, patients must present with a combination of the following: appropriate symptoms, positive clinical signs, and typical imaging findings.
Since each of these findings alone is nonspecific, the diagnosis of FAI syndrome requires their combination. It is crucial to note that there is not something like an asymptomatic FAI based on imaging alone.
In Cam morphology, the femoral head has an abnormal shape, often appearing more oval than spherical, which causes abnormal contact with the acetabulum.
This can lead to cartilage damage and hip pain, particularly during activities involving hip rotation or flexion.
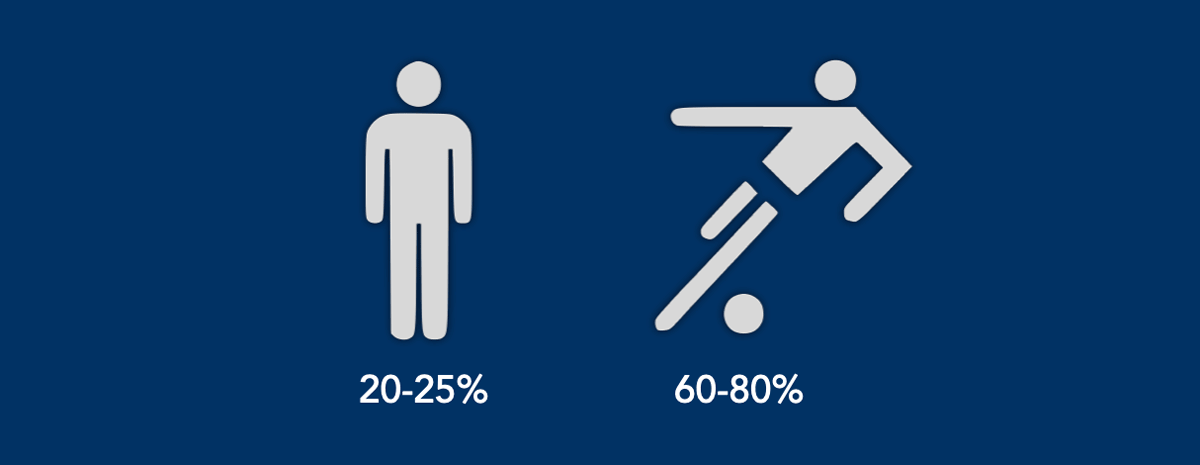
Cam morphology is especially common in athletes.
In a study of young professional football players, Cam morphology was observed in 60–80% of participants, compared to 20–25% in a control population.
Symptoms
Symptoms
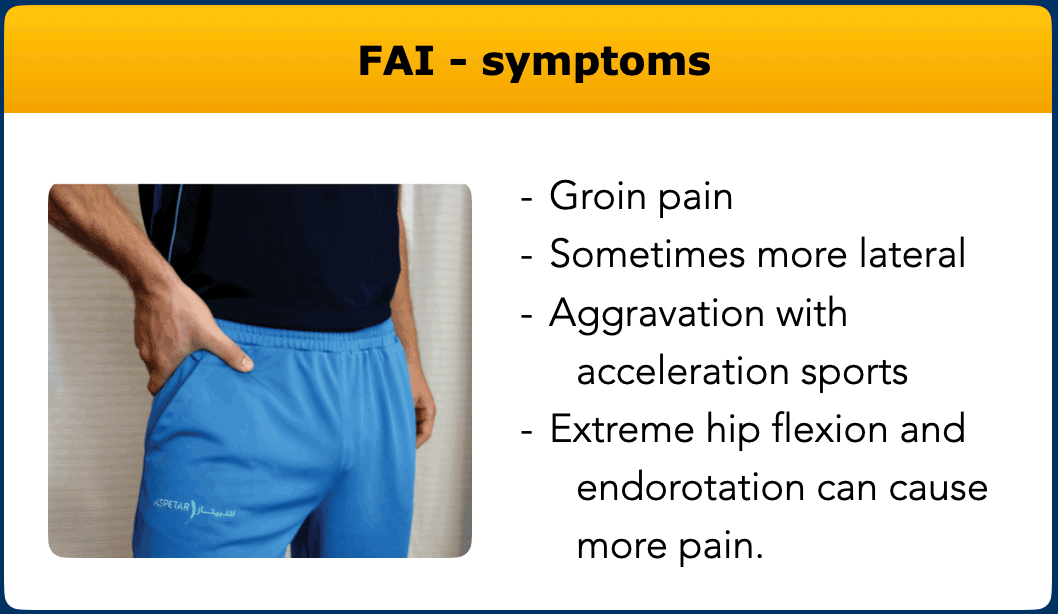
of the FAI-syndrome are moderate to marked hip or groin pain.
The patients
typically indicate the location of the pain by forming a “c-sign” with their hand,
as it is located deep within the hip.
There is aggravation of the complaints with acceleration sports as well as
squatting, climbing stairs and prolonged sitting.
Extreme hip flexion and endorotation can cause more pain.
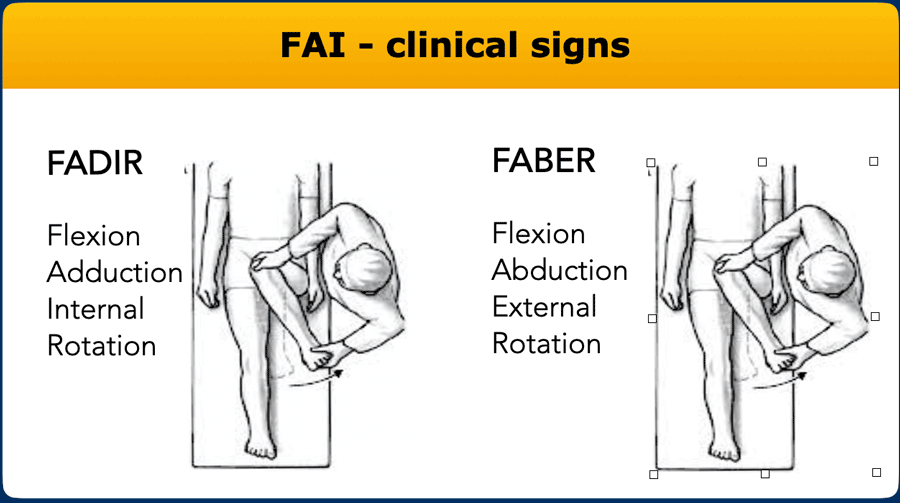
Clinical signs
Hip impingement tests usually reproduce the patient's typical pain.
There is often a limited range of hip motion, typically restricted internal rotation in flexion, especially if you compare to the contralateral side.
The FABER test is flexion combined with abduction and external rotation.
The most commonly used test is the FADIR test with flexion, adduction and internal rotation.
These tests are sensitive but not very specific and thus the typical symptoms and imaging findings should also be present to make the diagnosis of FAI.
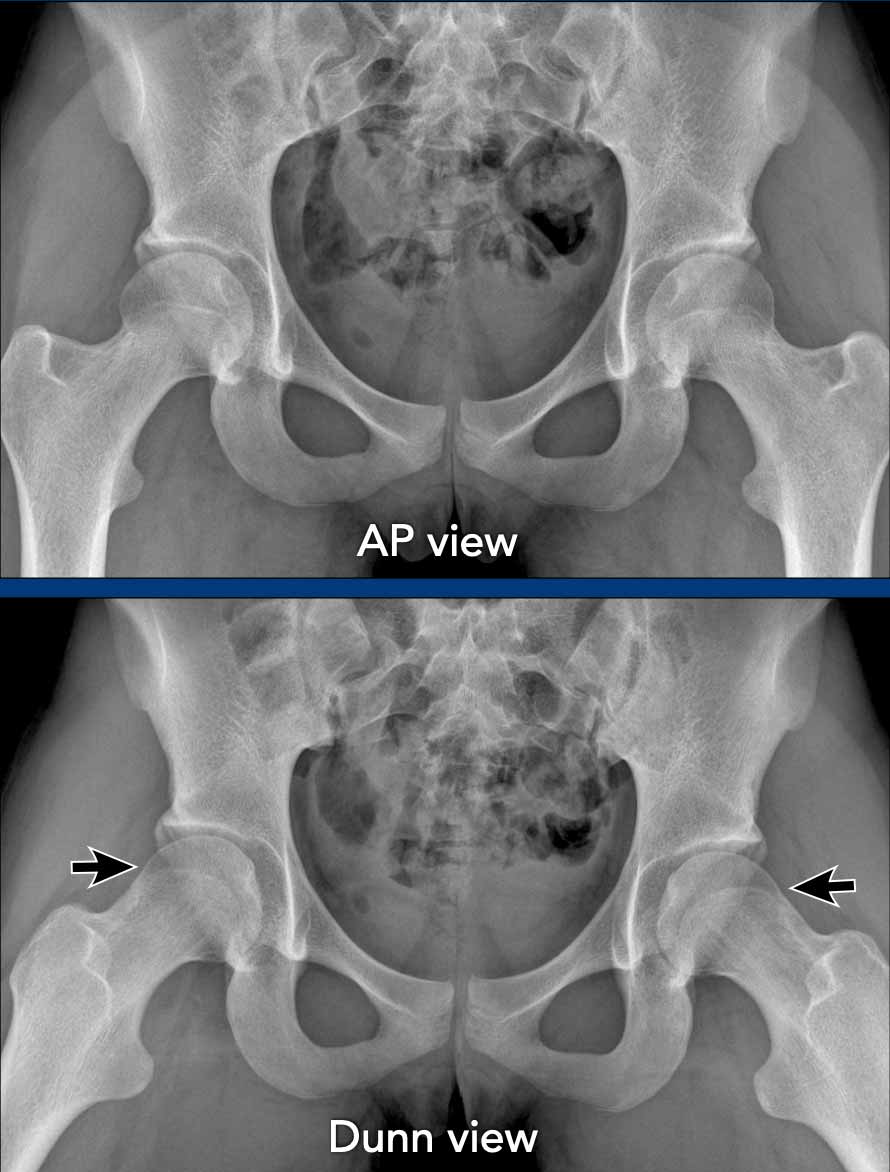
Dunn view
The Dunn view is an oblique view that helps to visualize the head-neck junction in a manner that is not typically seen in standard views like the anteroposterior (AP) or lateral views.
It is performed by having the patient lie on their back with their affected hip flexed at about 45° and abducted at 20° to 30° with neutral rotation.
This positioning allows for a clearer view of the anterosuperior aspect of the head-neck junction, which is often difficult to assess on standard views and is the most common location of the cam morphology.
Images
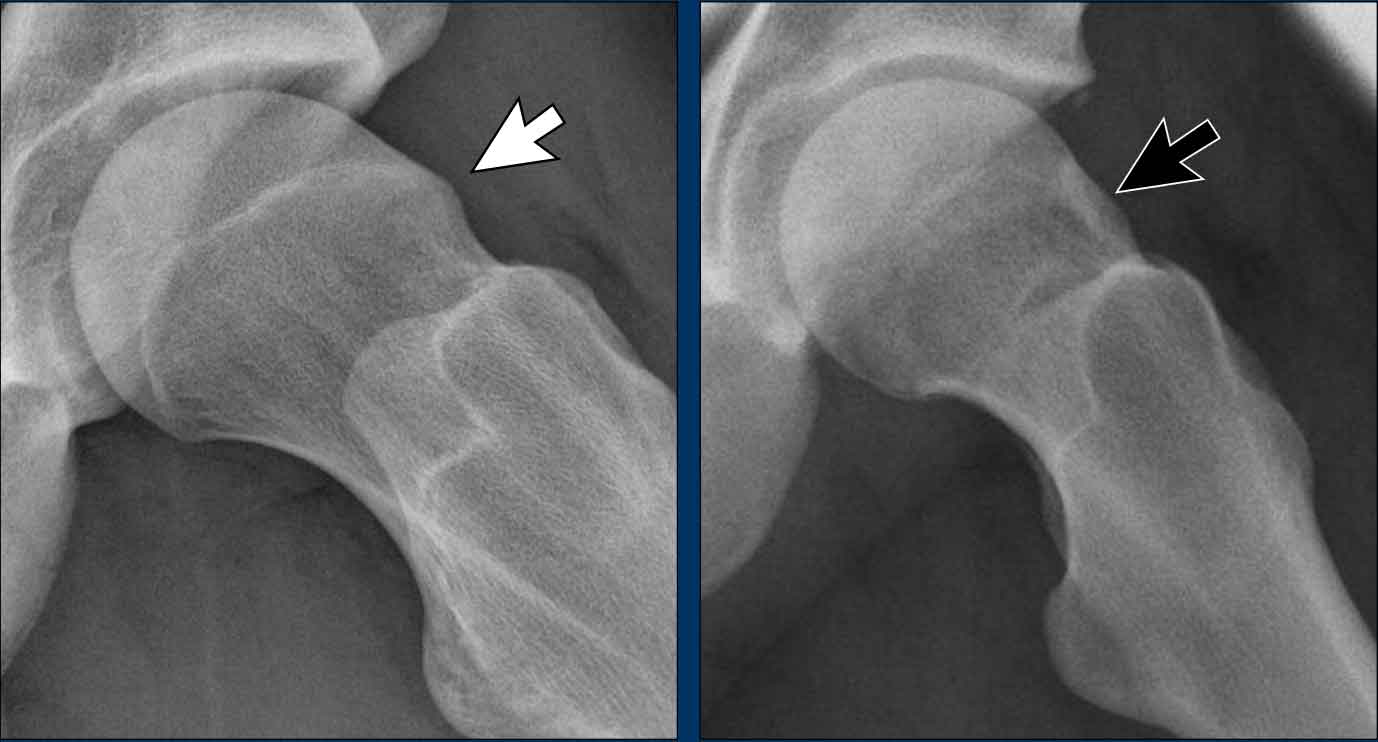
A 20-year-old gymnast with hip complaints.
On the AP view the femoral head-neck region looks normal.
On the Dunn view there is Cam morphology on both sides (arrows).
CAM morphology
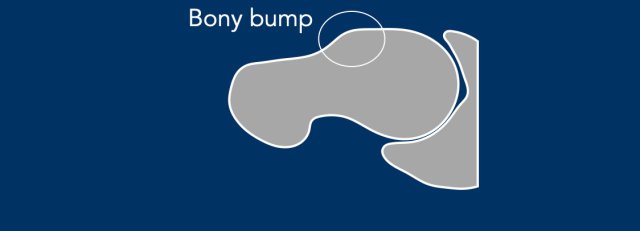
Cam morphology refers to a benign bony prominence that develops at the femoral head-neck junction of the hip often combined with an osseous asphericity of the femoral head.
This causes the femoral head and neck to rub against the acetabulum leading to damage of the labrum and cartilage and lead to hip pain, particularly with activities that involve hip rotation or flexion.
The international consensus is to refer to it as Cam morphology and to avoid terms such as Cam lesion, bony bump, or pistol-grip deformity, as it may also be present in many asymptomatic athletes.
When observing a bony bump or osseous convexity, as seen in the illustration, it can be referred to as Cam morphology.
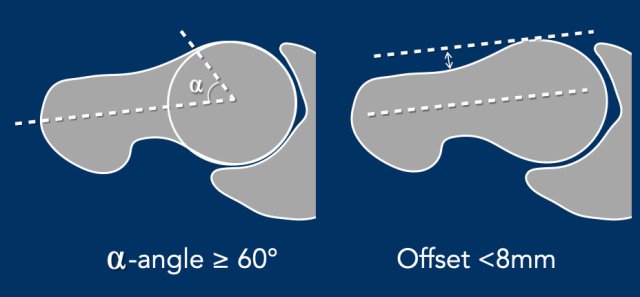
Alpha angle
The
alpha angle is measured by drawing a circle through the femoral head, a line
from the center of the femoral neck to the center of the femoral head, and then
a line from the center of the femoral head to where the femoral head-neck
junction intersects the circle.
If the angle is 60 degrees or more, it can be classified as Cam morphology.
This measurement can be used both on conventional imaging as well as
cross-sectional imaging - with cross-sectional imaging being more sensitive.
The threshold has been increased recently to 60 degrees to make it more
specific.
Offset
Additionally, the offset can also be measured on cross-sectional imaging (CT or
MRI).
For this, a line is drawn on the anterior side of the femoral head, parallel to
the femoral neck.
If the distance between this line and the anterior side of the femoral neck is
less than 8 mm, it can be classified as Cam morphology.
Alpha angle measurement
The normal hip shows an alpha-angle far below 60º.
The hip with the Cam morphology has an alpha-angle far above 60º.
Of course, when the Cam morphology is as pronounced as in this case, angle measurements are unnecessary.

This is a more subtle case of Cam morphology in a young male.
Notice that the epiphyseal plates have not yet closed (arrow).
Images
Two examples of Cam morphology.
Pincer morphology
Pincer morphology is characterized by an abnormal orientation or abnormal shape of the acetabulum, such as acetabular retroversion or acetabular protrusion. This results in excessive or abnormal coverage of the femoral head, which can lead to impingement.
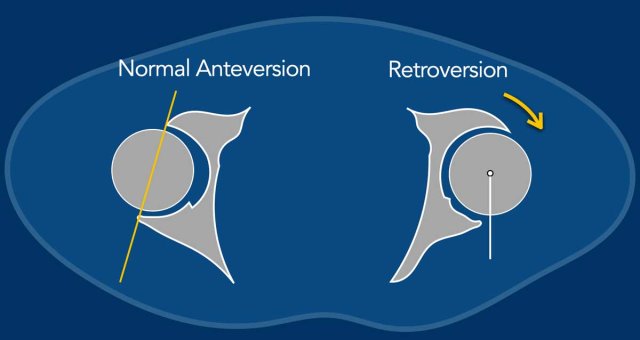
Acetabular Retroversion
The normal acetabulum has an anteverted orientation (figure), meaning it is more open on the anterior side compared to the posterior side. On radiographs, the anterior wall projects medially to the posterior wall.
In acetabular retroversion, the acetabulum is abnormally oriented, leading to excessive coverage of the femoral head on the anterior side, which can result in impingement during flexion and rotation. In addition the ischial spine will project more medially (ischial spine sign).
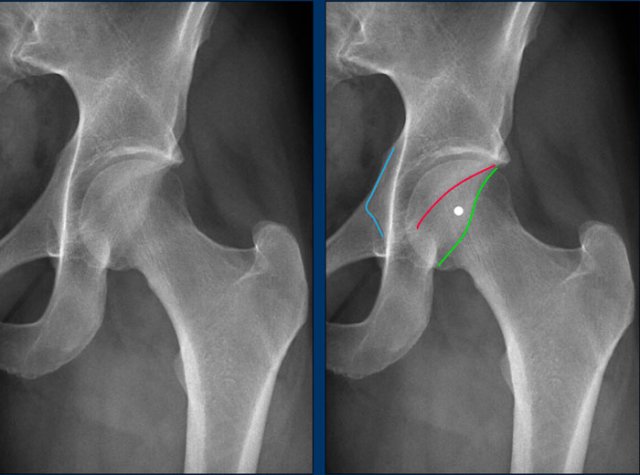
Normal anteversion of the acetabulum
This is a detail of the normal left hip on an AP Pelvis X-ray.
As a result of the normal anteverted orientation of the acetabulum, the border of the anterior wall (red line) projects medially to the posterior wall (green line) , i.e. no cross over.
The posterior wall projects laterally to the center of the femoral head, i.e. no posterior wall sign.
The ischial spine (blue line) does not project medially, i.e. no ischial spine sign.
Acetabular Retroversion
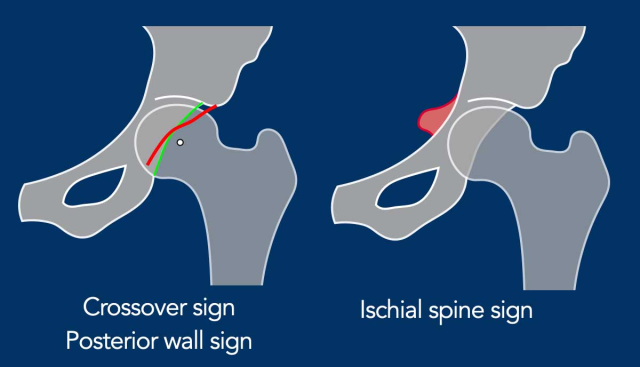
On radiographs, signs of acetabular retroversion include:
Cross-over sign - the anterior wall (especially the superior portion) projecting laterally to the posterior wall.
Posterior wall sign - the posterior wall projecting medially to the center of the femoral head.
Ischial spine sign - the ischial spine projecting more medially than normal.
If only the cross-over sign is positive, it is referred to as a focal (anterosuperior) pincer.
When
both the posterior wall sign and the ischial spine sign are also positive, it
is classified as a global pincer/acetabular retroversion.
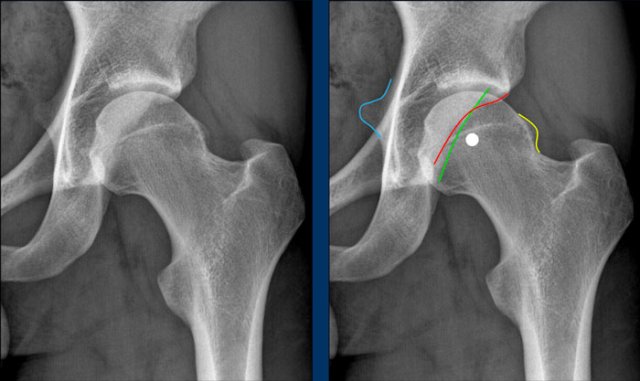
This is a detail of an AP Pelvis X-ray.
First study the image.
Then scroll to the next image.
Findings
- Cross-over sign - the superior portion of the anterior acetabular wall (red line) extends laterally beyond the posterior acetabular wall.
- Posterior wall sign - the posterior wall projects medially to the center of the femoral head.
- Ischial spine sign - the ischial spine projects more medially than normal (blue line).
These findings are consistent with acetabular retroversion, leading to a global pincer morphology.
Notice that there is also some cam-morphology.
This is another example of pincer morphology.
There is a subtle cross over sign.
In addition there is a posterior wall sign and ischial spine sign.
Notice that there is also cam-morphology (yellow line).
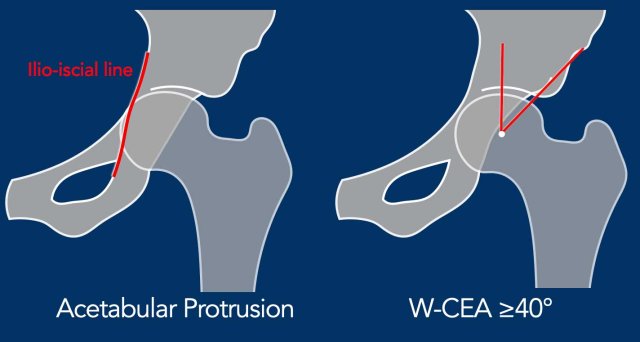
Acetabular protrusion
Ilio-ischial line
In acetabular protrusion, the acetabulum is too deep with inward displacement and global overcoverage of the femoral head. If the medial border of the femoral head extends beyond the ilio-ischial line, this is referred to as acetabular protrusion.
CEA angle
When
measuring the center-edge angle (CEA), the lateral boundary of the
anterosuperior wall/lateral border of the acetabular sourcil should be used, also known as the lateral center edge angle of Wiberg/W-CEA.
This can be recognized on an AP x-ray by using the lateral margin of the subchondral
sclerotic zone of the superior acetabulum.
When using the most lateral border
of the acetabulum (which is usually reflective of the border of the superolateral
acetabulum rather than the anterosuperior border), or the L-CEA, the coverage might
be overestimated.
If there is a retroversion of the (superior) acetabulum, the
W-CEA and L-CEA can be the same.
If this angle is equal to or greater than 40 degrees, it is classified as global pincer with overcoverage of the femoral head.

Hip dysplasia
Unrecognized hip dysplasia is sometimes clinically mistaken for FAI-related complaints.
Therefore, it is important to also report any potential undercoverage or dysplasia. (i.e. L-CEA < 20 degrees).
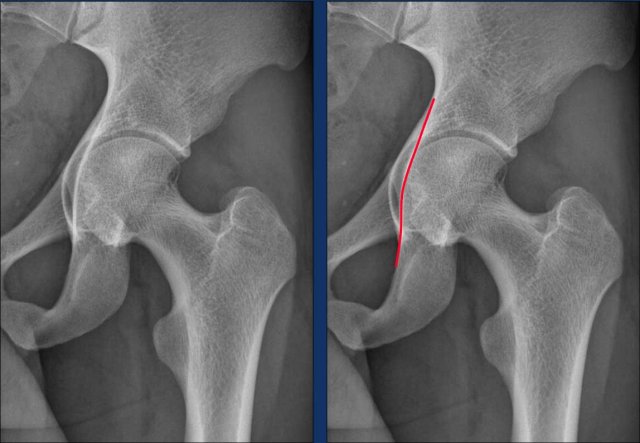
This image is of a 23-year-old male presenting with hip-related complaints.
Image
This is a subtle case of acetabular protrusion, where the femoral head slightly crosses the ilioischial line.

Image
Isolated pincer on both sides (only AP view available) with increased W-CEA in a 16 years old patient, who presented with hip-related complaints.
Treatment
Conservative therapy
In most cases, an initial attempt is made to alleviate symptoms through conservative therapy. This treatment involves providing insight into the origin of the symptoms, advising the avoidance of extreme postures, and, in the case of acetabular retroversion, exploring whether adjusting the pelvic tilt is feasible.
Arthroscopic therapy
If these measures prove ineffective, surgical intervention may be considered. Prior to surgery, an MR arthrography will be performed to assess the condition of the labrum and rule out other possible pathologies, such as osteoarthritis or idiopathic bone marrow edema, among others. Small labral tears are typically left untreated, while larger unstable tears may be either excised or repaired.
Images
In a patient with Cam morphology, the effect of reshape of the femoral head-neck junction is seen (arrow).
Examples of FAI

Combination of Cam and Pincer morphology
These images are from a 28-year-old woman who participates in CrossFit at a professional level. She has been experiencing complaints in the left hip region, specifically on the anterior side, for the past year. The symptoms worsen during squats and hip flexion.
Upon examination, there is reduced hip flexion (painful at 120°) and limited rotation (restricted to 20° and painful).
First study the radiograph.
Then continue with the detailed views...
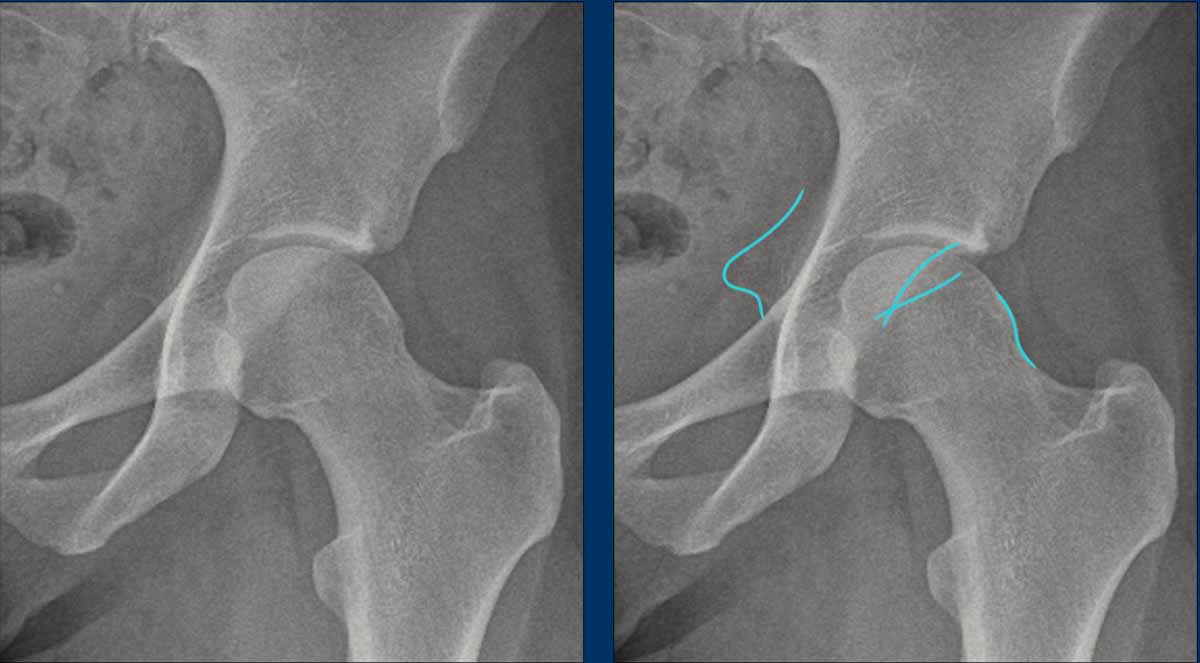
Although the findings are subtle, there is evidence of Pincer morphology, indicated by the crossover sign and ischial spine sign.
The retroversion of the acetabulum results in increased prominence of the ischial spine and leads to the superior portion of the anterior wall of the acetabulum overlapping the posterior wall on imaging.
Furthermore, there is a mild indication of Cam morphology.
Continue with the MR-arthrogram...
Subsequently, MR arthrography was performed, revealing a labral tear in the anterosuperior region.
Initially, the patient was treated conservatively with physiotherapy, but this did not lead to satisfactory results.
An arthroscopic procedure was then performed, involving a reshaping of the femoral head-neck junction (arrow), which resulted in significant improvement.

Cam and osteoarthritis
This is a 27-year-old man who sustained deep groin pain seven years ago while squatting.
Since then, he has stopped playing football but has continued to experience the pain.
Images
The radiographs reveal a bony prominence on the femoral head/neck consistent with cam morphology.
Continue with the MRI...
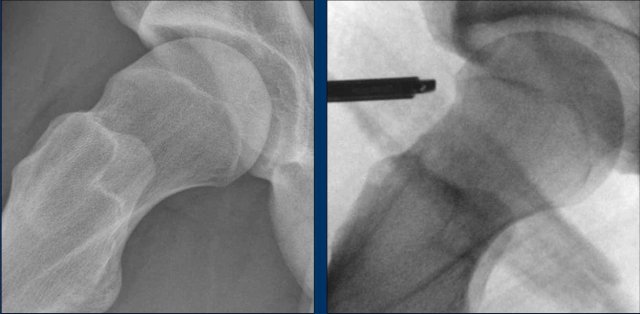
Images
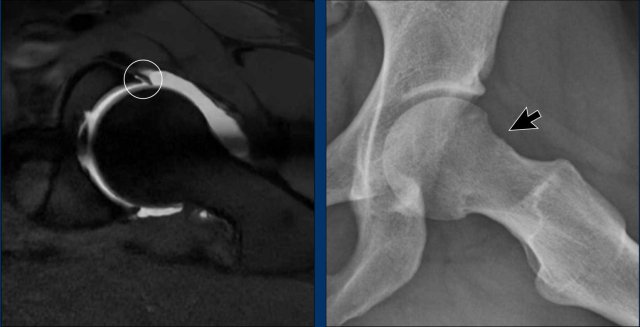
The
image on the left is a so-called bone/zero TE (ZTE) MRI.
It is a special MRI acquisition to study the bones.
The images look quite similar to CT images and can be made as part of a
MR-arthrogram of the hip.
It shows a small osteophyte (black arrow).
Scroll through the images of the MR-arthrogram on the right side.
There is a cartilage defect on the acetabular side (yellow arrow).
Conclusion
Since there is already osteoarthritis in this patient, he is not a candidate
for an arthroscopic treatment.
He was treated conservatively with physiotherapy.

Subspine impingement
Subspine Impingement is a condition in which the anterior inferior iliac spine, also known as the subspine, impinges upon the femoral neck or head, especially during activities requiring deep hip flexion or rotation, such as sports or yoga.
These images are of a 23-year-old woman with a history of rheumatoid arthritis.
She presented with progressive pain in the right hip, particularly during flexion movements while practicing yoga.
Images
There is a variant with a low position of the inferior iliac spine (arrow).

This is another example of subspine impingement in a 28-year-old amateur football player who sustained acute trauma to the right hip region eight months ago.
Since then, he has experienced progressive hip complaints.
Physical examination reveals significantly reduced flexion, as well as decreased internal and external rotation.
Image
There is a typical avulsion injury of the anterior inferior iliac spine at the insertion of the rectus femoris tendon.
This has resulted in bony overgrowth, causing impingement. on the femoral head/neck region.
The ossification was surgically removed.